The endocannabinoid system is a naturally occurring system within the brain. Researchers have been looking at CBD and THC, which can both be extracted from cannabis, as therapeutics. CBD and THC are chemically similar to the body’s endogenous (natural) endocannabinoids. Research has shown promising results, so doctors have been starting to prescribe medical marijuana to patients instead of alternative drugs. So how has this impacted drug abuse?

In The Brain
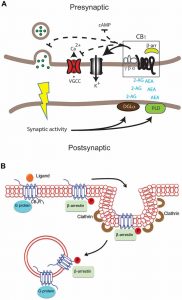
First, it is important to understand the endocannabinoid system (ECS) in the brain. The ECS has retrograde signaling and involves several receptors and ligands. Two of the major endogenous endocannabinoids (eCB) are Anandamide (AEA) and 2-Arachidonoylglycerol (2-AG). Also, the CB1 and CB2 receptors are the most prevalent receptors in this system. Both receptors are G-protein coupled receptors (GPCRs). This means that when a ligand binds, G-proteins are activated.
Activated CB1 and CB2 receptors result in a signaling cascade that releases neurotransmitters from the postsynaptic neuron which travels back to the presynaptic neuron. These signals then modulate the presynaptic neuron’s signaling, effecting all signaling done by the presynaptic neuron. The two major endocannabinoids, along with exogenous cannabinoids CBD and THC, bind to the cannabinoid 1 (CB1) receptor. The CB1 receptor is located on presynaptic neurons and mediates the central nervous system’s (CNS) effects. AEA and 2-AG activate the CB1 receptor, which regulates adenylate cyclase activity and inhibits cAMP, voltage-gated potassium channels, calcium channels, and neurotransmitter release.
Next is the cannabinoid 2 (CB2) receptor. The CB2 receptor is mainly found on microglia and is involved with the immune system, including inflammation. AEA and 2-AG are agonists for the cannabinoid receptors and are triggered by an influx of calcium at postsynaptic sites after synaptic activity. Overall, the eCB system mediates a variety of events including synaptic plasticity, learning and memory, pain perception, neuroprotection, inflammation and mood.
Medical Marijuana and Drug Abuse
As medical marijuana is becoming legal, doctors are switching to marijuana or CBD as a therapeutic in replacement of other medications. This is significantly decreasing the amount of addictions and overdoses for several reasons. First, the majority of people who get addicted to opiates were once prescribed them. So, instead of prescribing opiates for pain management, doctors are prescribing medical marijuana or CBD. Second, people who are already addicted to opiates are willingly switching to marijuana, therefore reducing the amount of addictions and overdoses. Same goes for anxiety prescriptions. Since marijuana and CBD have been shown to reduce anxiety, people are using it as a therapeutic instead of other medication that pertain to anxiety, such as Xanax. Further, showing a third way medical marijuana is reducing drug abuse. Lastly, marijuana has been shown to induce a “forgetting effect” by stimulating the part of the brain that controls memory. This can be helpful for people who are struggling with addiction by reducing cravings and reducing the memory related to drug use. Potentially, resulting in a fourth way medical marijuana is reducing drug abuse.
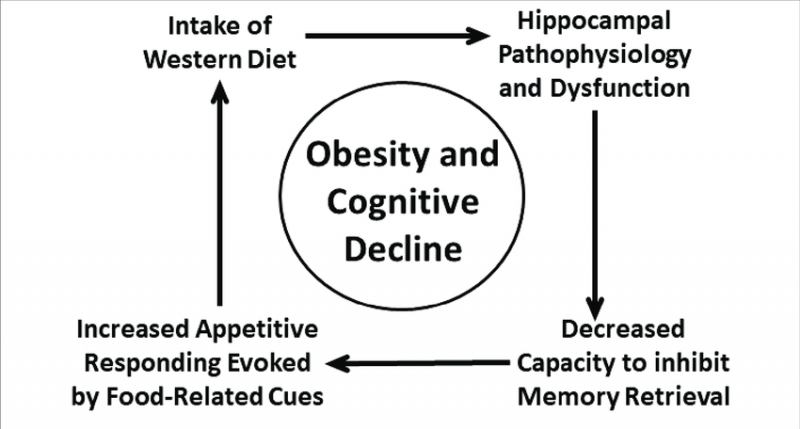
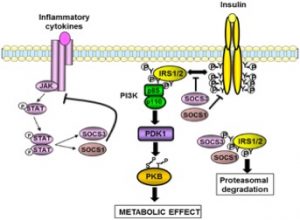
 disturbances, etc.), this appears to not be great for our overall health. These disturbances typically lead to a low grade, local inflammation of the gut, which then turns systemic. Because of the gut-brain connection, systemic inflammation becomes neuroinflammation, or inflammation of the brain’s tissue. This can have all kinds of adverse effects that can show themselves behaviorally, or change the way the brain functions. Since the gut can affect the brain negatively like this, there are also positives that can occur. One of the major upsides that research is looking into is that we may be able to address and treat issues that are commonly associated with the brain, such as anxiety and depression, through the gut.
disturbances, etc.), this appears to not be great for our overall health. These disturbances typically lead to a low grade, local inflammation of the gut, which then turns systemic. Because of the gut-brain connection, systemic inflammation becomes neuroinflammation, or inflammation of the brain’s tissue. This can have all kinds of adverse effects that can show themselves behaviorally, or change the way the brain functions. Since the gut can affect the brain negatively like this, there are also positives that can occur. One of the major upsides that research is looking into is that we may be able to address and treat issues that are commonly associated with the brain, such as anxiety and depression, through the gut. to neurodegenerative diseases such as Alzheimer’s disease or Parkinson’s. Basically, inflammation is really not great, and can cause a cascade of negative effects that can happen over a period of decades. The good news though, is that inflammation can be treated using endocannabinoids, but that also doesn’t mean we shouldn’t try to prevent inflammation in the first place.
to neurodegenerative diseases such as Alzheimer’s disease or Parkinson’s. Basically, inflammation is really not great, and can cause a cascade of negative effects that can happen over a period of decades. The good news though, is that inflammation can be treated using endocannabinoids, but that also doesn’t mean we shouldn’t try to prevent inflammation in the first place. 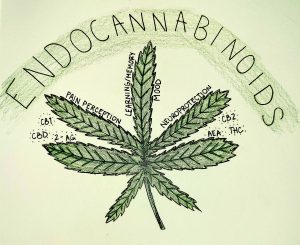

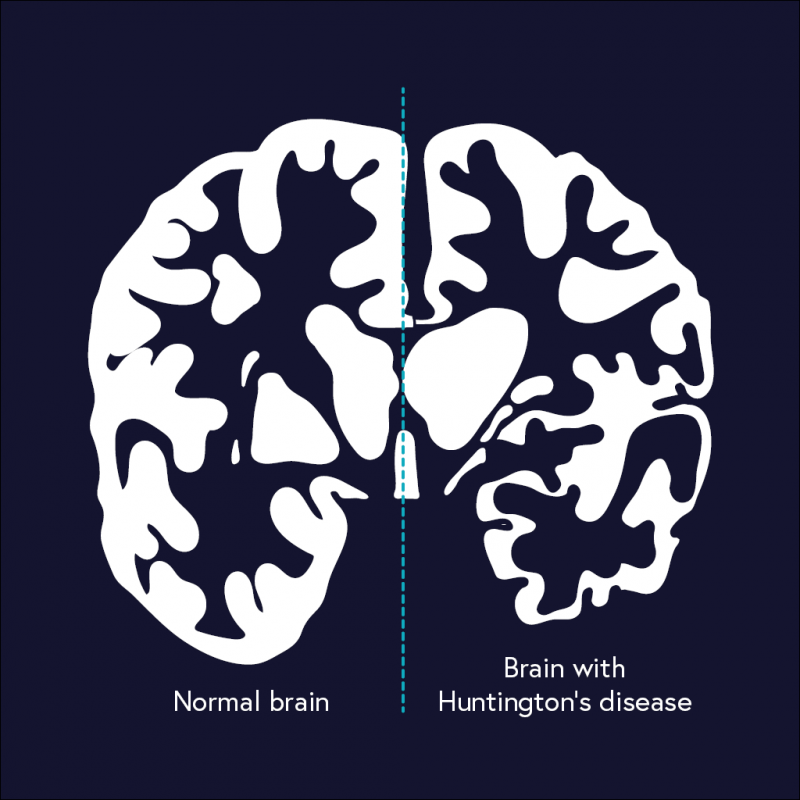
 Because the endocannabinoid system assists with memory, reduction of inflammation, and protection from neurodegeneration, it makes sense that dysregulation of the system could play a role in Alzheimer’s Disease. Evidence also supports a role of the system: levels of key molecules are off in AD brains and CB1 and CB2 receptors are correlated with tau tangles and other hallmarks of AD.
Because the endocannabinoid system assists with memory, reduction of inflammation, and protection from neurodegeneration, it makes sense that dysregulation of the system could play a role in Alzheimer’s Disease. Evidence also supports a role of the system: levels of key molecules are off in AD brains and CB1 and CB2 receptors are correlated with tau tangles and other hallmarks of AD.