
We’ve been struggling to name what trauma does to the mind for a long time. Civil War soldiers called it “soldier’s heart” — a cardiovascular condition, they thought, brought on by the stress of combat. WWI veterans were told they had “shell shock,” initially assumed to be literal brain damage from artillery blasts, until doctors noticed identical symptoms in soldiers who’d never been near an explosion. [1] After WWII it became “battle fatigue.” The name kept changing because the phenomenon was always slightly beyond our grasp. It wasn’t until 1980, pushed forward by a convergence of Vietnam veterans, Holocaust survivors, and sexual trauma survivors, that PTSD was formally recognized as a diagnosis. The DSM had actually dropped its predecessor diagnosis entirely in 1968. [1]
That long, halting history matters because it shapes how we think about the disorder today. PTSD isn’t one thing. The DSM-5 recognizes a dissociative subtype, characterized by feeling detached from oneself or from reality, alongside the standard diagnosis. [2] The ICD-11 goes further, formally recognizing Complex PTSD — typically following prolonged or repeated trauma — as a distinct condition, though the DSM hasn’t followed suit. [3] Researchers have also identified subtypes that don’t appear in any diagnostic manual: a “threat-reactivity” profile dominated by fear and hypervigilance, strongly associated with combat; and a “dysphoric” profile dominated by depression and emotional numbing, which appears more tied to pre-existing genetic vulnerability than to the type of trauma experienced. [4]
That last point raises an obvious question: if two people go through the same event and one develops PTSD while the other doesn’t, what’s actually different between them? The answer, neuroscience is beginning to show, is partly molecular.
A 2014 paper by Johannes Reul at the University of Bristol traced what happens in the brain during and after a psychologically stressful event, at the level of individual neurons. [5] When we encounter something threatening, the adrenal glands release stress hormones that travel to the hippocampus — the brain region central to memory formation. Reul’s team found that in a specific subset of hippocampal neurons, these stress hormones interact with a signaling pathway normally associated with learning to trigger a cascade of changes inside the cell (Figure 1).
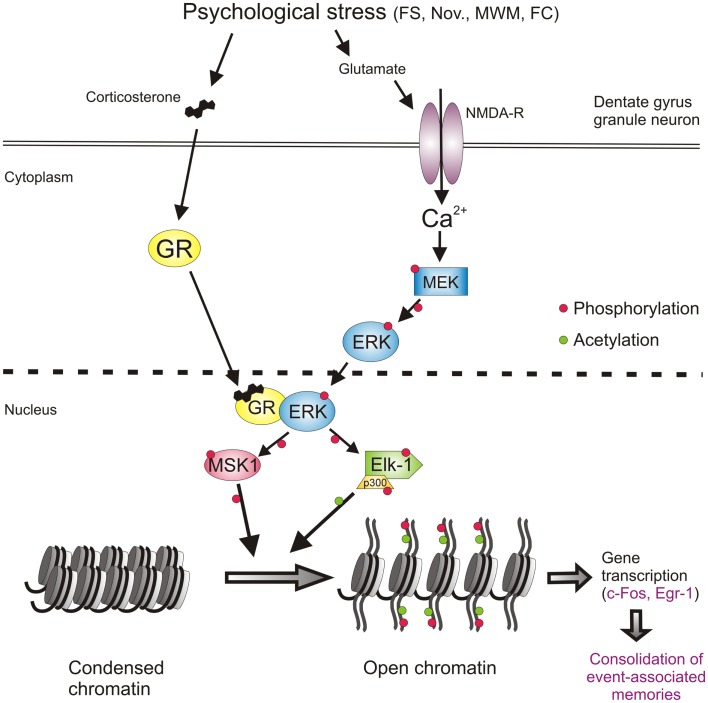
The cascade ends at the DNA itself: proteins that control which genes are accessible get chemically modified, switching on genes that drive long-term changes in how those neurons function. The stressful experience, in other words, leaves a physical mark on the genome of specific brain cells — a mark that shapes how the memory is encoded and stored.
Crucially, Reul’s research found that this process is gated by anxiety. The neurotransmitter GABA normally acts as an inhibitory brake on these neurons. When anxiety is high and GABAergic inhibition is correspondingly low, the neurons are more easily activated and the full molecular cascade is more likely to fire. In animal studies, drugs that boost GABA activity blunted the stress response at the molecular level; drugs that suppress it amplified the response dramatically. Voluntary exercise, which Reul’s group also studied, appeared to increase GABA synthesis over time and reduce the intensity of stress-induced molecular changes — a possible mechanism behind exercise’s well-documented benefits for anxiety and mood.
This connects the molecular picture back to the clinical one. Higher baseline anxiety means a lower threshold for triggering the memory-consolidation cascade, which may explain why anxious individuals face elevated risk for PTSD after trauma. It also suggests why the “dysphoric” research subtype — with its roots in pre-existing biology rather than trauma — might represent a distinct pathway into the disorder altogether.
For over a century, PTSD cycled in and out of official recognition, framed alternately as weakness, neurological damage, or simple failure to adjust. The 1968 DSM dropped the diagnosis entirely. What research like Reul’s provides is something that advocacy alone couldn’t: a biological explanation for why traumatic memory is different from ordinary memory. It isn’t a failure of resilience; it’s the product of specific, powerful processes in the brain that, under the right conditions, encode experience with unusual and sometimes lasting permanence. Understanding those processes is the first step toward one day being able to interrupt them.