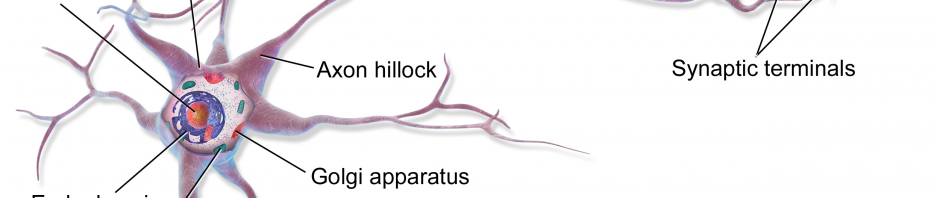
ALS, or amyotrophic lateral sclerosis, is a progressive neurodegenerative disease that affects nerve cells in the brain and the spinal cord.
After discussing our weekly article in our Neurochemistry class on ALS, I found this to be one of the most interesting but also quite saddening neurological diseases. I want to first lay out general facts that are important to ALS but also what the disease does to you overtime.
ALS, as stated above, is a fatal motor neuron disease where the average person with the disease only makes it a few years due to respiratory failure. Nerve cells start to die and degrade and cause sclerosis or essentially hardening in the spinal cord leading to muscle atrophy or failed muscle movements.
Most people with this disease have it because it being sporadic, but about 10% of people genetically inherit the disease. You can test for it genetically then if that’s the case. The disease is a painless progress, but things that start giving evidence that you may have it include: tripping, dropping things, abnormal fatigue in appendages, slurred speech, muscle cramps, and weirdly enough, uncontrollable periods of laughter or crying. Regarding respiratory failure, people with ALS typically receive assistance in breathing with a permeant ventilator due to respiratory muscles like the diaphragm.
Currently, there is one main drug that inhibits glutamate release which is called Riluzole. It works to assist breathing but does not help everyone that takes it. The drug extends ALS patients lives by a few months. Besides that, treatment for ALS typically is just weakening the side effects like reducing muscle cramps or fatigue—There is no cure for this disease.
Yeah, I would have to say so far from what I said, ALS sucks. All diseases suck, but I would argue this is one the worst. First, you get all this muscle weakness and you start to need assistance from others around you to do normal things. Getting through that hoop is plenty, but throwing on top that you only will live on average a few years after diagnosis? Knowing there is no cure?
Yeah all neurological diseases have NO cure. Some of those diseases eat away at you mentally and you forget maybe who your significant other is, like seen in types of dementia This motor neuron disease isn’t targeting you mentally but only physically. So, you start as a grape and end as a raisin, but indirectly I would argue you are being affected mentally. YOU are aware of everything. You see yourself deteriorate, you see yourself slowly become less and less social because you communicate less. You watch your family and friends help you, help you so far until the decision is life or death. There’s that point where you can’t even blink or move, but inside your head your thoughts and ideas fly—do you get to choose what happens next?
ALS: A Brief Background & Why It…Sucks.