
I am very glad that I was able to take NeuroChem as my capstone course because I feel that it was one of the only capstones that I wouldn’t have any trouble being interested in. After hearing from friends how the class was structured I thought that it sounded interesting to be able to learn about a new neurological disease every week. Now after having completed the class I found it to be rather enjoyable and successful as a capstone experience. I found that every week I was looking forward to our new research articles and learning how these different neurological diseases work and possible ways that they can be treated. I felt the our class was a great class because we had a nice wide range of disciplines in the class with chem majors, bio majors, and some psych majors all able to contribute their own unique knowledge base and way of thinking. All our points of view put together allowed me to look at these diseases in different ways that I wouldn’t have before. I also felt that I was able to bring in the knowledge that I have accumulated from my biology and chemistry background allowing me to better understand the chemical pathways of these diseases. I also found that after taking this class I better understand the breadth and severity of some of the different ailments that face millions of people and actually found that in a lot of cases if people knew more about these ailments that they could maybe be prevented or hopefully further studied in order to find potential treatments. I would for sure recommend this class to anyone interested in science, medicine or the brain to take this class as their capstone course because I really did learn a lot about different neurological diseases but I also learned how to read through difficult material and get the most information out of it that I could in order to understand the pathway of the diseases we went through the class.
Farewell to my Loyal Readers (if there are any)

Dear Faithful Readers,
I’d first off like to thank you all for your wonderful loyalty to me and my blogs. Not once did one of you reply to my posts telling me I am a dipstick or a complete fool. Thanks, you really know how to make a kid feel good. I’d also like to thank you for coming along with me on this journey throughout my capstone experience in this my senior year at Concordia College. This class was completely different for me compared to any other that I’ve taken and I’ve got to be honest, I loved it. If you would so indulge me one last time, please let me explain.
The basic format of a lecture is to sit back, shut up and let your professor tell you everything there is to know about their discipline. I am not saying you can’t ask questions and voice your opinion, but it isn’t as common when there’s 30 kids vigorously writing notes trying to keep up. Questions or comments only tend to drive out one of two thoughts that’s on everyone’s mind; either “shut the hell up so we can keep moving” or “thank God someone asked.” This class however was very different. There were no traditional lectures. Everyone was on the same level. The professor was just another student and we did our best to teach each other and develop critical thinking and generate thought-provoking discussions. Every week we would tackle a new review article about a neurological disorder and learn about current research surrounding it. Every article was difficult to understand at first but as a team we tackled every single one and developed the best understanding we could. Once we developed a good understanding of the article, discussion would take place.
Every Friday we would meet and form discussion groups and we’d have guided discussions about everything you can imaging surrounding each disorder. Everything from the scientific basis for a disorder to public policy regarding it, we covered it all. We then would take our discussions and final thoughts and share them with you, our fellow neighbors and friendly readers. We hoped to engage all of you with thought-provoking questions and ideas that sparked interest in learning more about the world we live in. Some of you may have even read about disorders that affect someone close to you and maybe then you were able to better understand that person, maybe not. We hope that with our critical thinking and active engagement with you as readers allowed for more awareness to spread about current issues surrounding these disorders.
Science is commonly a topic which the general public doesn’t really understand. I honestly believe the basic framework of how science is taught is to blame for this. Scientists are experts in what they study and have so much knowledge to offer the world about their findings however they’re incapable to do so in an understandable way. Concordia’s curriculum and the framework of this capstone course prides itself on developing good scientists who can bloom into experts in their field but more importantly, can accurately and successfully communicate that knowledge to those that need it; you, our neighbors and friendly readers. Thank you so much for following along and please, take time to learn more about the world around you any way you can. If you think the world is a beautiful place now, wait until you start to understand it more.
Take Care,
Sebastian
For the longest time, whenever I heard that someone was having a migraine and was unable to do a certain task, my initial reaction was along the lines of… “Well that sucks, but pop some Excedrin, drink a lot of water, and get back to it!” For individuals that have never had a migraine before — like myself — the condition may seem like merely an awful headache. However in reality, the effects reach farther than mere head pain. Symptoms such as nausea, vomiting, photophobia and phonophobia are often felt by those afflicted by this troublesome neurovascular disorder. Because none of my family members are affected by migraines and the condition is typically genetically linked (to some degree), I have never, and hopefully never will understand what migraine headaches feel like. However, after learning about what is physically going on in the brain during a migraine attack, I have a much greater respect for those afflicted.
The cause of migraines is still under dispute, and for many, the trigger is very different. Some can be set off by light while others can be set off by sound, etc. A host of different environmental factors can be attributed to causing migraines. However, despite the trigger, the effects are triggered by similar systems and occurrences in the brain.
There are several different structures and systems within the brain have been identified as primary culprits in migraine symptoms. One hypothesis suggests that migraines are triggered by abnormal levels of CGRP (calcitonin gene related peptide) released into the bloodstream, triggering excessive vasodialation and stimulation of nearby sensory neurons, inducing pain. However the cause of excessive CGRP release is still unknown. The nerve that is most commonly affected is the trigeminal nerve, a cranial nerve with three branches (opthalmic, maxillary, and mandibular) supplying sensory information to parts of the face and head. When CGRP floods the vessels in the head followed by vasodialation, the sensory components of the trigeminal nerve become overactive, causing extreme pain.
Recent drugs such as triptans and gepants have been used to treat migraines, however both have their ups and downs. Triptans work by by causing vasoconstriction and reducing CGRP (causes of the condition) however considerable side effects have been observed such as dizziness, nausea, fatigue, chest symptoms and paresthesia, deterring many from taking the medication. Gepants work by blocking the CGRP receptor. Although they are effective for those who experience side effects of triptans, they can be expensive.
For those who like myself have never experienced a migraine before and see it as just a bad headache, STOP! The condition is very debilitating for those afflicted. Without sufficient knowledge about the condition and what can be done to treat it, additional research must be done to give those with migraines much needed relief.
The Need for a New Migraine Treatment
Migraines are a debilitating neurovascular disorder characterized by frequent headaches, nausea, and sensitivity to light and/or sound among other symptoms. The exact cause of migraines is still unknown but researchers know how some of the symptoms arise and how to target them for treatment. Because it is a neurovascular disorder, the blood vessels in the brain, particularly the Middle Meningeal Artery (MMA), are a big part of the etiology of migraines. When vessels such as the MMA become inflamed and dilated, it can trigger the start of a migraine. This leads to further inflammation of the area around the vessel which leads to the long-lasting headaches felt by migraine sufferers.
Although it is not really known for sure how inflammation of a cerebral blood vessel can cause all of the symptoms seen in migraines, it has become a target for drug makers in an effort to curb the effects of this devastating disorder. Common migraine treatments involve the use of several different drug types. Triptans are used to combat the inflammation and dilation of blood vessels such as the MMA. They work by activating serotonin receptors on the blood vessel to constrict it, as well as serotonin receptors on nerve endings surrounding the vessel to inhibit the release of pro-inflammatory signaling molecules. Because triptans are only treating the dilated and inflamed vessels they are not useful as a precautionary drug and only alleviate the symptoms once they being to take hold.
Some drugs that are in development now to be taken as preventative for migraines involve gepants and glutamate antagonists such as Topiramate. These medications bypass the blood vessel and act directly on the nerve endings to damping their signaling. This, in theory, inhibits the pain reception so migraines are more bearable. The problem with these drugs is that it is not addressing the problem and only working to damping the sensations felt during a migraine. The future of viable migraine treatment hinges on research into the cause of the inflamed blood vessels and a way to stop them from happening in the first place.
More Than Just a Headache
Many people suffer from migraines each year. They can quickly put an end to your day as every sound, sight, and touch can cause nauseating pain. Many people have to take time off from work for migraines and it can drastically reduce one’s daily activities. They can even become dangerous when a sudden attack occurs while driving. What makes them so intense though? Why are they so much more than just your regular headache, and why does it seem like some people will get them twice a week, while others may never have a migraine their entire life?
In order to understand why migraines are so much worse than a regular headache, we must first know what it happening during a migraine. Like many brain disorders, scientists have not yet located the source that triggers a migraine. This is because many migraines are slightly different and the trigger that initiates them can be different for each individual. They do have a good understanding of what occurs during a migraine though and that has helped them treat the symptoms of a migraine.
During a migraine neuropeptides are released into the blood vessels that surround the brain. Since the actual brain doesn’t have pain receptors, the headache pain you feel during a migraine is due to the pain receptors connected to these surrounding blood vessels. One of the neuropeptides released is CGRP. CGRP is responsible for dilation of these vessels and also causes inflammation to occur. When inflammation occurs it over sensitizes the nerve that relays pain from the vessels to the brain called the Trigeminal Nerve. When this nerve is over sensitized it will send intense pain signals when only mildly stimulated. This is what causes most of the migraine symptoms such as pain when sneezing, coughing, bending over, and anything else that may increase pressure in the head and set off this sensitized nerve.
Ways that they have begun treating migraines is by using medications that reduce the dilation and inflammation of CGRP. Two drugs that hinder the effects of CGRP are Triptans and Gepants. Another method is to block the signal sent by the Trigeminal Nerve. This can be done by using Botulin, the chemical used in Botox, which paralyzes the nerve temporarily.
Hopefully scientists will continue to advance in their knowledge of migraines in order to reduce the suffering of those affected by them. Migraines can keep an individual from their daily responsibilities such as work, school, or taking care of their children. Hopefully discoveries in the future will help these people live a life free of this painful ailment.
Migraines
I have done some pretty stupid stunts in my life. I have jumped out of moving vehicles at 30 mph, I have broken toes while playing volleyball and continued playing barefoot, I have dislocated a pinky and popped it back in, I have had multiple concussions, I have grabbed electric fences, I have stabbed my foot with a fork, I have jumped off a barn, I had swine flu, in short I had quite the interesting teenage years.
It is with all of this qualification that I can rightfully say none of these things hurts nearly as bad as having a migraine. This is an ailment that makes even light hurt terribly. This is the sort of pain that forces you to lie in bed for days, only to arise so that you can puke. This is not the sort of pain that one can just simply “tough it up and work through,” it is completely debilitating. Because of this, it is easy to see that this would be a heavily researched area of science.
Our paper discussed that migraines are likely caused by vasodilation in the brain. This means that the blood vessels that supply blood flow to the brain are carrying more blood than they normally do. This is caused by, and conversely causes a multitude of reasons/symptoms.
This vasodilation can sometimes cause something called an Aura. An Aura is commonly experienced as a visual disturbance. Imagine staring into the sun for a couple minutes and then trying to look somewhere else, that is essentially what an aura looks like. Auras do not have to be visual however, they can be associated with hearing, smell and deja vu or jamais vu. These auras, in whatever form they come, usually arrive minutes to hours before a migraine attack begins. They are your body’s little pleasant reminders that you are about to be destroyed from pain radiating behind your eyes.
There is not currently any “cure” for migraines. However, many medicines can help alleviate the symptoms. Hopefully, research in the future will lead to a powerful and robust treatment for this detrimental illness.
Migraines: I Wouldn't Wish Them On My Worst Enemy
Migraines are a debilitating illness that can stop the sufferer in its tracks. Unlike other diseases we have talked about thus far in my Neurochemistry class, this is one that I can relate to directly because I suffer from them. It is hard to explain the intense pains and sensations that come with my migraines to other people. In my case, my migraines come on about once every month and leave me helpless for hours at a time. The pain is so severe that sleep doesn’t even come to relieve me. I wouldn’t wish them on my worst enemy.
It is hard to explain ones migraines to other people that have them as well because everyone experiences them differently. People have different symptoms, different things triggering their migraines and the duration of their migraines are not the same. It is these factors that are making the life of scientists that are trying to research migraines difficult along with the fact that they don’t have effective laboratory markers nor animal models to be able to study them extensively. What we do know though is common symptoms of migraines include sensitivity to light and noise, nausea, vomiting and throbbing pain in the head. These painful headaches usually happen to those between the ages of 20 and 50 years old and as of yet there is no official cure for them.
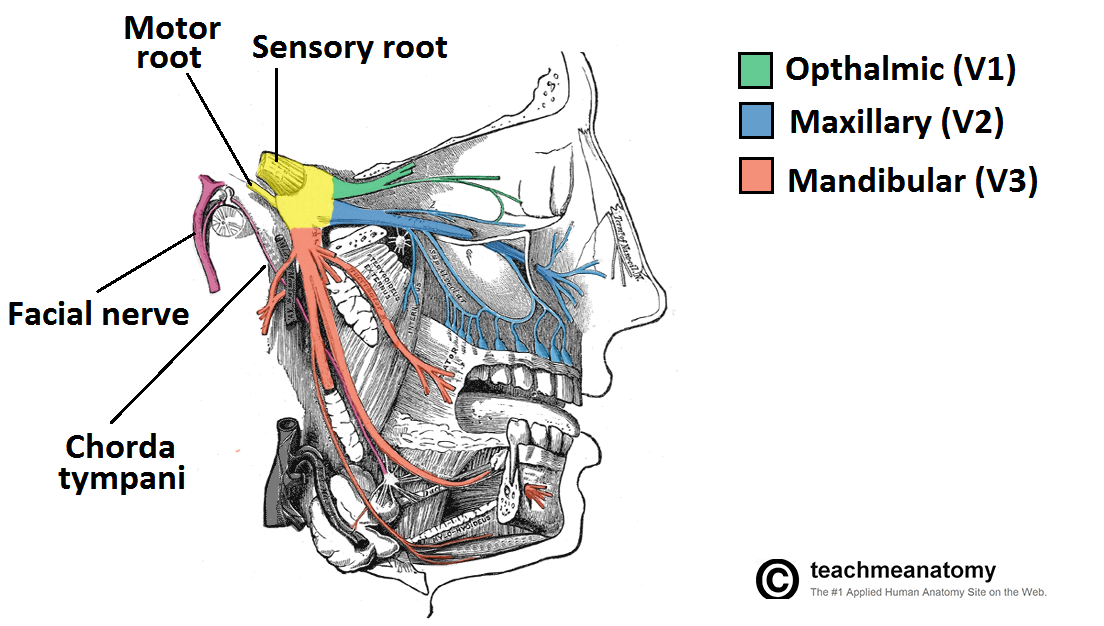
Science does not know exactly what causes migraines but have some insight into them. What they think occurs during a migraine attack is the vasodilation of cerebral blood vessels. It is theorized that this vasodilation occurs in response to the release of Calcitonin Gene-Related Peptides (CGRPs), ultimately affecting the trigeminal nerve. CGRPs are produced in the peripheral and central nerves and results from alternative splicing of the calcitonin gene. It has been found that along with CGRPs, other molecules such as serotonin, bradykinin, histamine, and prostaglandin are thought to affect sensory neurons around the trigeminal nerve, causing pain. The trigeminal nerve is the fifth cranial nerve. It is full of sensory neurons and its job is to transmit sensations from the face to the brain. As the name indicates, there are three branches to this nerve and they are the ophthalmic, maxillary and mandibular. The ophthalmic provides sensory innervation to the forehead, upper eyelid, cornea, bridge and tip of nose, the nasal cavity and the front half of the scalp. The maxillary provides sensory innervation to the cheeks, lateral nose, upper lip, upper jaw, the teeth and upper oral cavity. Lastly the mandibular provides sensation to the lower teeth, lower jaw, lower oral cavity and lower face. It is the ophthalmic nerve that researchers believe is the most affected during migraine attacks due to its location being where the largest amount of pain is felt in the majority of these attacks.
As I said before there is not that much that is known about migraines as a whole besides theories and thoughts as to what causes them. There are been research looking into the genetic components but unfortunately there has been nothing found that links migraines together besides those that have familial hemiplegic migraines (FHMs). FHMs are a form of migraine headache that is an autosomal dominant trait that runs in families. The gene mutations that are associated with FHM are CACNA1A (FHM1), ATP1A2 (FHM2) and SCN1A (FHM3). All three of these genes encode for ion channels or an ion pump, suggesting that there is a loss in the balance of ions that could be disrupting the normal release of neurotransmitters in the brain. It is important to reiterate though that FHM is the ONLY type of migraine that has a genetic link that has been found. Researchers are hoping that a better understanding of FHM could lead to a better understanding of common migraines as a whole.
Migraines are crippling to experience and I would not wish them onto anybody. Though there are medications out there that lesson the intensity of migraines once they have already started as well as hopefully prevent them, there is no known treatment that completely cures them. According to the Migraine Research Association over 10% of the US population is affected by migraines. With its high rate of prevalence, and selfishly for my own sake, I hope that further research will be able to someday yield concrete information on this extremely painful illness. Migraines are extremely traumatic and the less one has to suffer from them, the better.
Picture Found At: http://teachmeanatomy.info/wp-content/uploads/Overview-of-the-Anatomical-Distribution-of-the-Trigeminal-Nerve-and-its-Terminal-Branches.png
Additional Resource: http://www.migraineresearchfoundation.org/fact-sheet.html
Migraines and the Hope for a Cure
Like a blurry dream in the back of my mind, the thought of my first ever migraine lingers. I had just finished the longest run of my cross country career on a bright, blue-skied Saturday morning. Feeling abnormally tired, as to be expected, I headed home from the park where I began and ended my run. Upon arrival at home I ate my breakfast like usual, slowly sinking into what would be the worst headache of my life. Not much later I began to feel warm, tired, and complacent. In short time. My vision would start to go blurry, especially in my peripherals. It appeared as though fans were spinning all around me, fading my vision and destroying my depth perception. And then came the debilitating pain: the thumping when I was laying still, and sharp sting when I tried to move. Not knowing what was going on, I went to the clinic after only a couple hours, which had felt like days.
Migraines are a rather common problem in the United States, affecting over ten percent of the entire population. Yet although so common, very little is understood about the causes of migraines. The most recent research suggests that migraines are the result of various genetic changes in the brain affecting ion channels, in addition to some environmental factors. However, possibly the best hypothesis we have now is that pain results from migraines due to abnormal levels of calcitonin gene-related peptide released from vasculature in the brain. One of the main players in the migraine story is the trigeminal nerve, one of the cranial nerves that supplies a large portion of the face. The trigeminal nerve has been shown to have receptors for calcitonin gene-related peptide, and when they are blocked pain from migraines dissipates. It has also been shown that triptans, molecules that bind to 5-HT receptors in the brain, help relieve migraine symptoms and normalize the levels of calcitonin gene-related peptide. As a result, 5-HT receptor agonists, as well as calcitonin gene-related peptide receptor antagonists, are being used as possible drug approaches for migraine treatment.
Fortunately for me, my migraine subsided after rehydration and some rest suggested by the doctor. Only one time since have I experienced the migraine-like symptoms that tore me to pieces that Saturday morning a few years ago. Although much more work is needed, I am hopeful that a solid, standard treatment for migraines is on the horizon, as new research slowly solves this neurological mystery. Using our most recent discoveries, we can put an end to this problem that affects so many.
Migraines and the Bad Case of Vasodilation
As someone who has been fortunate to never have experienced a migraine, it can be difficult to understand what makes them so brutal. Migraines are more than just your typical headache. They include extremely-painful throbbing of the head, vomiting, nausea, and sensitivity to light and sound. They can be so severe that they are actually debilitating and can last for hours to days. It can prevent a person from attending work or school. Some people affected by migraines even experience auras before the full onset of the migraine. Auras can include flashes of light, blind spots, tunnel vison, tingling of the limbs, or even hearing sounds. Migraines themselves are difficult to treat and understand because they affect each person differently. In addition, unlike many other diseases and disorders of the brain, migraines come and go. They are not a “constant thing” that can be studied easily.
Vasodilation seems to be the main component behind the pain associated with migraines. Neuropeptides – in particular CGRP (calcitonin gene-related peptide) – are released from nerves and cause vasodilation of blood vessels in the cranium. When these blood vessels dilate, it activates the sensory neurons in that same area. It is the activation of the sensory nerves that cause the severe pain. In the head, the main sensory nerve affected with migraines is the trigeminal nerve, one of the twelve cranial nerves. This nerve has three main branches – the ophthalmic branch, the maxillary branch, and the mandibular branch. The trigeminal ganglion, which houses the cell bodies of the neurons that make up the trigeminal nerve, is the main source of CGRP in the trigeminal system. What is actually causing this release of CGRP and the migraine in the first place remains unknown, however. More research is necessary to help determine the cause so we can figure out the best way to prevent and treat migraines.
How, then, are migraines treated right now? Pharmacologically, drugs can be administered to help prevent migraines and help the migraines subside. Triptans are used to treat migraines already in progress and work by acting on serotonin receptors. The drugs are agonists of the receptor and reduce inflammation and cause vasoconstriction of the blood vessels, as well as reduce release of CGRP. Another type of drug, called gepants, can be used to prevent migraines. These drugs work by being an antagonist of the CGRP receptor. Although these drugs are helpful in treatment of migraines, they sometimes can be extremely expensive, limiting who is able to afford them or willing to pay a great deal for them.
It is important that we continue research and put more emphasis on migraines because they can be so debilitating. 12% of the US population suffers from migraines and the pain, vomiting, and sensitivity that is associated with them. It is more difficult to treat migraines, since they are a come-and-go-type disorder, but that does not mean we should put less into research about them. For some, living a life with severe migraines eliminates their ability to go to school, work, or take care of a family. They are confined to a dark, quiet room in hopes that the pain will go away. For those people, developing a better way to treat migraines – or even prevent them – is not only important, but essential.
The Headache That is a Migrane
We’ve all have had headaches, but most of his haven’t experienced the excruciating pain of a migraine. Some of the typical symptoms of a migraine include throbbing pain in head, nausea, vomiting, diharrhea, and pain behind one eye. The progession of migranes are broken into four stages (prodrome, aura, attack, postdrome)

There is no known cause of migraines, only theories. There are suggestions of ion channel dysfunction. The most popular idea that researchers propose is that migraines are the results of vasodilation of the extracranial arteries. This dilation can cause inflammation that triggers pain receptors on the trigeminal nerve. The trigeminal nerve is the fifth cranial nerve. It is broken into three branches. The first is the ophthalmic branch that supplies sensory innervation to forehead, front half of scalp, upper eyelid, cornea, bridge and tip of nose, and nasal cavity. The second branch is the maxillary branch that supplies sensory innervation to cheeks, lateral nose, upper lip, upper jaw, teeth, and upper oral cavity. The third branch is the mandibular branch, which provides sensory to lower teeth, lower jaw, lower oral cavity, lower face. This nerve also provides sensory to parotid gland, anterior 2/3 of tongue, and motor to muscles of mastication. If the trigeminal pain receptors are activated in a migraine, this explain the unilateral pain across the forehead that many experience.
Right now, doctors are treating migraines with three different types of medication. They include triptans, gepants, and glutamate agonists. Triptans are in the family of tryptamine based molecules. They are preventative and only treat a single migraine at a time. They cause constriction of blood vessels and inhibit some of the pro-inflammatory responses. Gepants are CGRP-agonists. The final drug type is glutamate antagonists. These inhibit AMPA and L-type receptors. This causes cells to depolarize slower.
We need to continue our research into the causes of migraines and drug treatments, because many people have migraines. This neurological disease causes a lot of pain, and can disrupt their everyday life. Through this research, we could even find more effective ways to treat normal headaches.
Resources:
https://moodle.cord.edu/pluginfile.php/390952/mod_resource/content/4/pathophysiology%20of%20migraine.pdf
http://neurochemistry2014.pbworks.com/w/page/89149016/Basic%20mechanisms%20of%20migraine%20and%20its%20acute%20treatment
http://en.wikipedia.org/wiki/Migraine
http://debbieupton.com/products-page/migraine-symptoms/