Cannabis
Cannabis is a generic term used for the variety of products derived from the cannabis sativa plant. Cannabis goes by many names including marijuana which describes parts of the plant high in THC[1]. Delta 9 tetrahydrocannabinol (THC) and Cannabidiol (CBD) are the most investigated[1]. Marijuana is one of the most used drugs in the United States, particularly among individuals aged 18-25.[1] In 2021, 35.4% of people aged 18 to 25 reported using marijuana in the past year[1]. The drug is surrounded by a significant amount of controversy and stigma as it is slowly being legalized for recreational use across the nation.
It is important to note that not all uses of marijuana are recreational. Before the drug was legalized for recreational use, it was legalized for medical use. Cannabis has been used in medicine to treat chronic pain, opioid withdrawals, seizures, multiple sclerosis, and decreased appetite[2]. The two main cannabis-derived medications available are Cannabidiol and Dronabinol[2].
Epidiolex
Epidolex (cannabiniol) is used in the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome. The medication is approved for individuals 2 years and older. it contains a purified form of CBD derived from marijuana without any THC. Epidiolex is administered orally with strawberry flavoring. Common side effects include drowsiness, diarrhea, decreased appetite, lack of energy, sleep problems, increased liver enzymes, and infections
Dronabinol
Dronabinol is commonly used to treat weight loss in individuals with AIDs. It is also used to treat nausea and vomiting associated with chemotherapy. Dronabinol is a synthetic form of THC. The medication can be taken as a pill ranging from 2.5-5mg of THC per dose. It can also be administered orally as a spray with a 2.7 mg/100ul dose. Common side effects include dizziness, euphoria, nausea, vomiting, stomach pain, paranoia, sleepiness, and abnormal thinking[4].
Cannabis use disorder
Cannabis use disorder is a mental health condition where cannabis use causes distress or impairments in day-to-day tasks and functioning. In more severe cases the diagnosis can be classified as cannabis addiction [5].
Symptoms
- Strong urge to consume cannabis
- Unsuccessful attempts to limit cannabis use
- Disruptions in social, occupational, or recreational activities because of cannabis use
- Developing a tolerance
- Confusion
- Delusions
- Memory issues
Long term effects
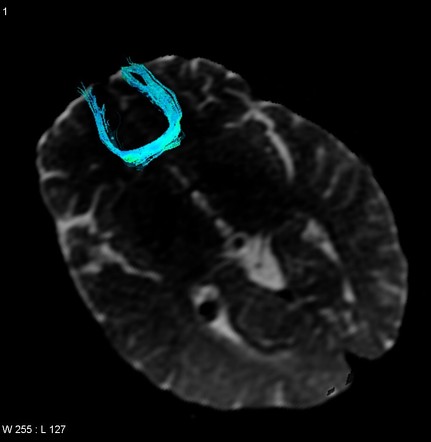
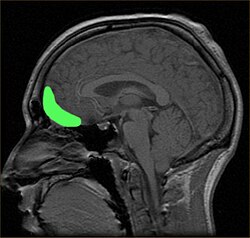
In the study Long-term effects of marijuana use on the brain, researchers found that long-term marijuana use had significant impacts on cognition and brain anatomy. Cannabis users exhibited significantly lower gray matter volume in the right and left middle orbitofrontal cortex (Figure 3) than controls. The marijuana groups also displayed increased white matter growth in the Forceps minor (Figure 4). Marijuana users also displayed significantly lower IQ scores compared to the control group.
[1] WHO. (2024, October 24). Cannabis. World Health Organization. https://www.who.int/teams/mental-health-and-substance-use/alcohol-drugs-and-addictive-behaviours/drugs-psychoactive/cannabis
[2] Cleveland Clinic medical. (2025, February 21). Marijuana. Cleveland Clinic. https://my.clevelandclinic.org/health/articles/4392-marijuana-cannabis
[3] Abu-Sawwa, R., & Stehling, C. (2020). Epidiolex (Cannabidiol) Primer: Frequently Asked Questions for Patients and Caregivers. The Journal of Pediatric Pharmacology and Therapeutics : JPPT, 25(1), 75. https://doi.org/10.5863/1551-6776-25.1.75
[4] Drugbank. (2025, February 16). Dronabinol: Uses, interactions, mechanism of action | drugbank online. https://go.drugbank.com/drugs/DB00470
[5] Cleveland Clinic medical. (2025a, February 21). Cannabis use disorder. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/cannabis-use-disorder
[6] Filbey, F. M., Aslan, S., Calhoun, V. D., Spence, J. S., Damaraju, E., Caprihan, A., & Segall, J. (2014). Long-term effects of marijuana use on the brain. Proceedings of the National Academy of Sciences of the United States of America, 111(47), 16913–16918. https://doi.org/10.1073/pnas.1415297111
[7] https://en.wikipedia.org/wiki/Orbitofrontal_cortex
[8]Gaillard F, Murphy A, Hacking C, et al. Forceps minor. Reference article, Radiopaedia.org (Accessed on 25 Feb 2025) https://doi.org/10.53347/rID-4705