
What is Psychopathy?
Psychopathy can be characterized as an individual who has shallow emotional response, lack of empathy, impulsivity and an increased likelihood for antisocial behavior. No this does not mean that one day of being emotionless or not wanting to have emotions makes you a psychopath. There are a lot of components going into a psychopathic diagnosis. One interesting statistic is that by Hare’s psychopathy checklist-revised, psychopaths make up around 20% of the prison population in North America.[1] Considering this statistic, psychopaths are prone to violence and usually have increased aggressive behavior therefore commit a greater number of violent attacks compared to non-psychopaths.[1]
There is a possible relation to having a certain gene increasing susceptibility to psychopathy. An individual could inherit a specific genetic pathway toward psychopathy which is associated with low-expression variant of Monoamine Oxidase (MAO-A) gene. The MAO-A gene functions to encode an enzyme that degrade dopamine, norepinephrine, and serotonin. There has been research on the MAO-A polymorphisms tied to short allele and psychopathic and antisocial traits.[2]
Psychopathy versus Antisocial Personality Disorder
Psychopathy: psychopaths characterized as selfish, domineering, irresponsible, impulsive, fearless, shallow, as well as lacking empathy and remorse. Not restricted to people showing criminal or deviant behavior, therefore may also be found in “socially well-adjusted and successful individuals”.[4]
Antisocial personality Disorder: characterized as lack of self-control (prefrontal cortex), low avoidance of punishment and negative stimuli (amygdala), and heightened sensitivity to rewarding stimuli (striatum).[4]
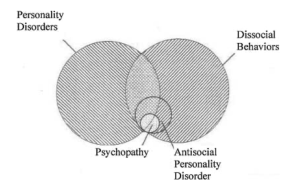
Figure 1: Comparison of antisocial personality disorder and psychopathy as they relate to Dis-social behaviors and personality disorders.[4]
What is going on in the brain?
In psychopathy it was found that there are deficits in frontal, temporal, and subcortical limbic structures of the brain. Overall, there was reduced amygdala function found in adult psychopaths and a failure of top-down regulatory control of ventral PFC. Therefore, emotional blunting was found in those diagnosed as psychopaths. Along with this the amygdala, commonly known for control of processing fear, plays a role in the emergence of aggressive behaviors sometimes associated with psychopathy as it has been found that the amygdala is smaller in those with psychopathy. For violent or aggressive behaviors, there could also be a correlation to reduced glucose metabolism in the corpus callosum. Interestingly enough, the striatum which consists of caudate, putamen, nucleus accumbent, and globus pallidus is found to be enlarged by 9.6% in psychopaths.[3] Lastly, psychopathy is associated with substance abuse, or that sensation-seeking behavior, which could produce orbitofrontal impairments.
Possible correlations to alcohol…
During the in-womb development it has been noted that consumption of alcohol could be associated to increased childhood aggression. This as evidenced by a “longitudinal study of over 100,000 men documented that prenatal nutritional deficiency is associated with a 2.5 fold increased risk for Antisocial Personality Disorder in adulthood”. Interestingly enough, certain nutrient deficiencies have been associated with aggressive and antisocial behavior including low levels of omega-3 and zinc which play a role in building up omega-3 fatty acids critical for neural development. Early brain maldevelopment could be due to reduced zinc levels which involves the amygdala and hippocampus.[3]
Overall, there are a lot of components that go into how to screen for psychopathy. With around 1-2% of the adult general population with this diagnosis, psychopathy is a prominent mental health disorder compared to other psychological diagnoses.[1]
Work Cited
- Anderson NE, Kiehl KA. Psychopathy: developmental perspectives and their implications for treatment. Restor Neurol Neurosci. 2014;32(1):103-17. doi: 10.3233/RNN-139001. PMID: 23542910; PMCID: PMC4321752.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4321752/#:~:text=Psychopathy%20is%20a%20neuropsychiatric%20disorder,antisocial%20deviance%20and%20criminal%20behavior
- Frazier A, Ferreira PA, Gonzales JE. Born this way? A review of neurobiological and environmental evidence for the etiology of psychopathy. Personal Neurosci. 2019 Oct 23;2:e8. doi: 10.1017/pen.2019.7. PMID: 32435743; PMCID: PMC7219694.
- Raine A. (2018). Antisocial Personality as a Neurodevelopmental Disorder. Annual review of clinical psychology, 14, 259-289. https://doi.org/10.1146/annurev-clinpsy-050817-084819
- Weber, S. Habel, U., Amunts, K., Schneider, F. (2008). Structural brain abnormalities in psychopaths – a review. Behavioral Sciences & the Law, 26(1), 7-28. https://doi-org.cordproxy.mnpals.net/10.1002/bsl.802.






 The barcode hypothesis is often brought up. A unique characteristic about GPCRs is that phosphorylation occurs and that determines their roles downstream. It also gives the guide for how or which beta arrestin binds to the GPCR. Phosphorylation can cause the GPCR to be inhibited, it can cause activation of other membrane receptors, one
The barcode hypothesis is often brought up. A unique characteristic about GPCRs is that phosphorylation occurs and that determines their roles downstream. It also gives the guide for how or which beta arrestin binds to the GPCR. Phosphorylation can cause the GPCR to be inhibited, it can cause activation of other membrane receptors, one 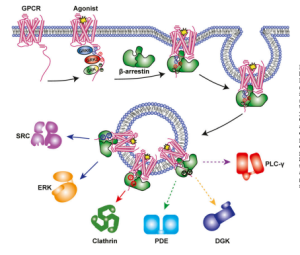
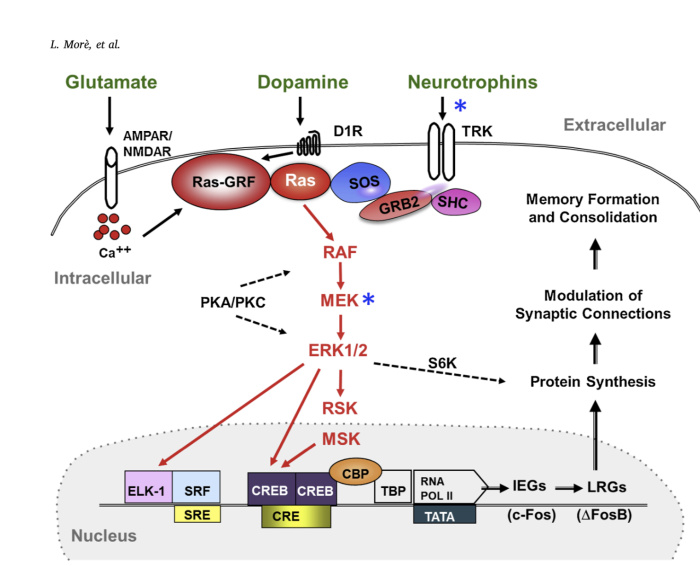

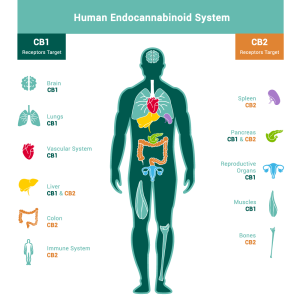
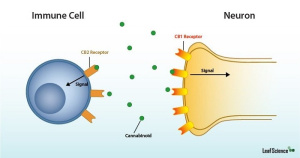

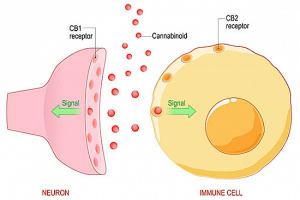
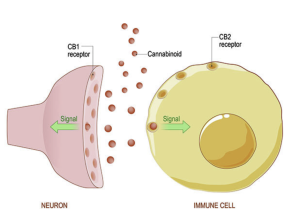
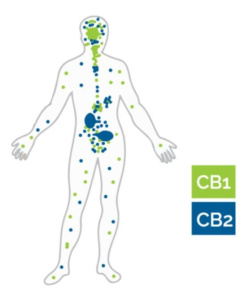
 Now that we know what the key players are, what exactly is the endocannabinoid system used for? The endocannabinoid system (ECS) has emerged as one of the key regulatory mechanisms in the brain that controls many events such as mood, pain, perception, learning, and memory. It may also provide a neuroprotective role in brain injury as well as potentially playing a role in drug abuse and dependence.
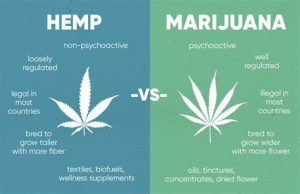
Now that we know what the key players are, what exactly is the endocannabinoid system used for? The endocannabinoid system (ECS) has emerged as one of the key regulatory mechanisms in the brain that controls many events such as mood, pain, perception, learning, and memory. It may also provide a neuroprotective role in brain injury as well as potentially playing a role in drug abuse and dependence.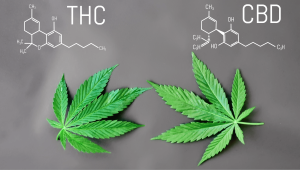 Let’s talk drugs, such as cannabis (better known as marijuana, pot, weed, grass, dope). Cannabis is a psychoactive drug from the actual cannabis plant. There are two main components of the cannabis plant.
Let’s talk drugs, such as cannabis (better known as marijuana, pot, weed, grass, dope). Cannabis is a psychoactive drug from the actual cannabis plant. There are two main components of the cannabis plant.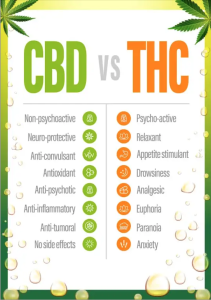 One major difference between these two is that CBD is legal in all 50 states whereas THC is only legal (or decriminalized) in 22 states. There are also more forms of CBD than that of THC.
One major difference between these two is that CBD is legal in all 50 states whereas THC is only legal (or decriminalized) in 22 states. There are also more forms of CBD than that of THC. It can be seen that white people and people of color are using marijuana at the same rate, but people of color (specifically African Americans) are arrested for violating marijuana possession laws at nearly
It can be seen that white people and people of color are using marijuana at the same rate, but people of color (specifically African Americans) are arrested for violating marijuana possession laws at nearly 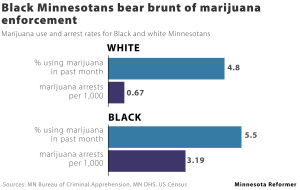
 While CBD is legal in 50 states there are still interesting statistics that can be talked about! Roughly
While CBD is legal in 50 states there are still interesting statistics that can be talked about! Roughly 
{kind=link}
{kind=link}
{kind=link}