Having read a number of articles within my neurochemistry course, mostly related to neurological conditions and cognitive diseases, it appears inflammation is a significant and central component. This made me wonder if inflammation is a significant factor in other conditions as well. This week’s article answered my question suggesting a link between hypothalamic inflammation and obesity. The general gist of the article explains that inflammation of the hypothalamus impairs energy balance and contributes to insulin resistance which through a number of pathways leads to the development of obesity through altered neurocircuitry.
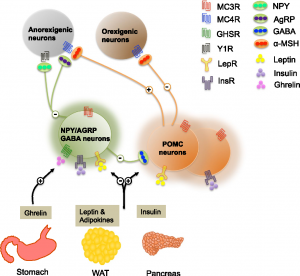
Image indicating relationship between signaling pathways of Ghrelin, Leptin, & Insulin.
The hypothalamus is a region of the brain critical in the regulation of eating and drinking, body temperature and energy maintenance, memory and stress control, and regulator of the endocrine system. Because of its significant roles, inflammation of the hypothalamus could result in dysregulation within these functions yielding several unfavorable events such as the development of obesity.
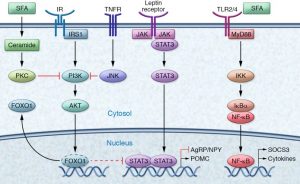
Molecular signaling & interactions related to development of obesity
Typically within a healthy individual, there is a balance between the signaling of leptin, ghrelin, and insulin. The leptin receptor when activated stimulates a protein abbreviated as Stat through a cascade of signaling. When Stat is activated, it moves into the nucleus of the cell and activates the transcription of proteins. Stat activates a protein abbreviated as POMC ( an appetite suppressor) and inhibits another abbreviated as AgRP ( an appetite stimulator) which signals satiety and suppresses the desire to feed. When activated, the insulin receptor, also through a cascade of signaling, activates a series of proteins (abbreviated respectively as IRS1, Grb, SoS, PI3K, and Akt) that stimulate the molecule that follows leading to the final activation of Akt. Akt similar to Stat, enters the nucleus of the cell but activates a protein abbreviated as Foxo which typically blocks the activity of Stat preventing the sensation of satiety and allowing for feeding when necessary. When Foxo is activated by Akt, it leaves the nucleus of the cell and is unable to inhibit Stat which allows for the sensation of satiety when necessary and stops the feeding behavior. These pathways help to regulate the intake of nutrients and maintenance of a healthy weight. Ghrelin works similarly but ultimately stimulates AgRP to elevate hunger and encourage feeding when the body requires more energy and nutrients.

Balance vs imbalance in hypothalamic signaling in obesity
Issues arise when an individual consistently consumes a high-fat and unhealthy diet, specifically those consisting of high concentrations of saturated fatty acids. Generally speaking, unsaturated fatty acids are healthier than saturated fatty acids as saturated fatty acids can stack upon one another and lead to clots or cholesterol buildup within arteries. A general rule of distinction between these two types of fat is that saturated fats are typically solids at room temperature while unsaturated fats are typically liquid. When consistently consumed in high concentrations, saturated fatty acids activate receptors abbreviated as TNF-alpha and TLR4. These receptors also use a cascade of signaling and activate JNK which phosphorylates (in this case inhibits) IRS1 blocking insulin signaling and NF-kappa-B which activates another protein (SOCS) which inhibits both insulin and leptin signaling. With disruptions in both insulin and leptin signaling, ghrelin becomes the primary stimulator leading to increased feeding, dysregulation of the sensation of satiety, and imbalances with energy maintenance leading to increased and continued storage as fat.
The challenges of obesity are not only limited to the molecular implications but society as a whole. With increased access to unhealthy foods, increasing prices of fresh produce, and the time commitment to create a healthy and well-balanced meal, temptations sway in the direction of fast, cheap, and easy. Advancements in technology decrease the amount of energy we expend throughout the day as food can be delivered to our door, we sit for hours on end, and we pursue the use of technology and entertainment over physical labor and exercise. Obesity and so many of the conditions we face go beyond just the molecular implications and often include an environmental or societal component as well. To truly address these matters; we must confront the influencing factors, both the micro and the macro. Thanks for reading.
 The way the brain controls appetite and food cravings changes substantially after consuming foods high in fat. Like many “bad” habits, eating high-calorie, high-fat foods can be difficult to stop once you’ve become accustomed to the diet—
The way the brain controls appetite and food cravings changes substantially after consuming foods high in fat. Like many “bad” habits, eating high-calorie, high-fat foods can be difficult to stop once you’ve become accustomed to the diet— The
The 

 It has been found that there are a number of ways in which food, specifically food that is high in fat, can have addictive qualities. In some ways this assertion is already intuitive, as you never just want to have
It has been found that there are a number of ways in which food, specifically food that is high in fat, can have addictive qualities. In some ways this assertion is already intuitive, as you never just want to have  drug addicts, where cortical brain regions involved in executive control and decision making have been heavily implicated. Through eating a high fat diet, we might be allowing our brains to think that eating more high fat items is what should occur.
drug addicts, where cortical brain regions involved in executive control and decision making have been heavily implicated. Through eating a high fat diet, we might be allowing our brains to think that eating more high fat items is what should occur. 

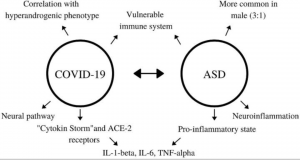
 agile balance that is maintained between estrogen, progesterone, and the androgens. This hormonal imbalance often results in the development of cysts within the ovaries, contributing to irregular menstrual cycles, infertility, and anxiety/depression. Additionally, overproduction of these androgens leads to excess hair all over the body, acne, and insulin resistance and obesity.
agile balance that is maintained between estrogen, progesterone, and the androgens. This hormonal imbalance often results in the development of cysts within the ovaries, contributing to irregular menstrual cycles, infertility, and anxiety/depression. Additionally, overproduction of these androgens leads to excess hair all over the body, acne, and insulin resistance and obesity.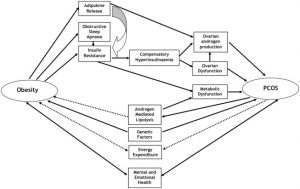


 to the infection reaches the fetuses blood circulation supply. Some responses, such as certain antibodies, can be helpful to building the fetus’s immune system, but others, like cytokines, can harm the fetus’s
to the infection reaches the fetuses blood circulation supply. Some responses, such as certain antibodies, can be helpful to building the fetus’s immune system, but others, like cytokines, can harm the fetus’s 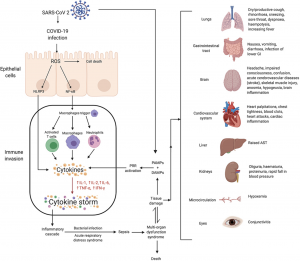

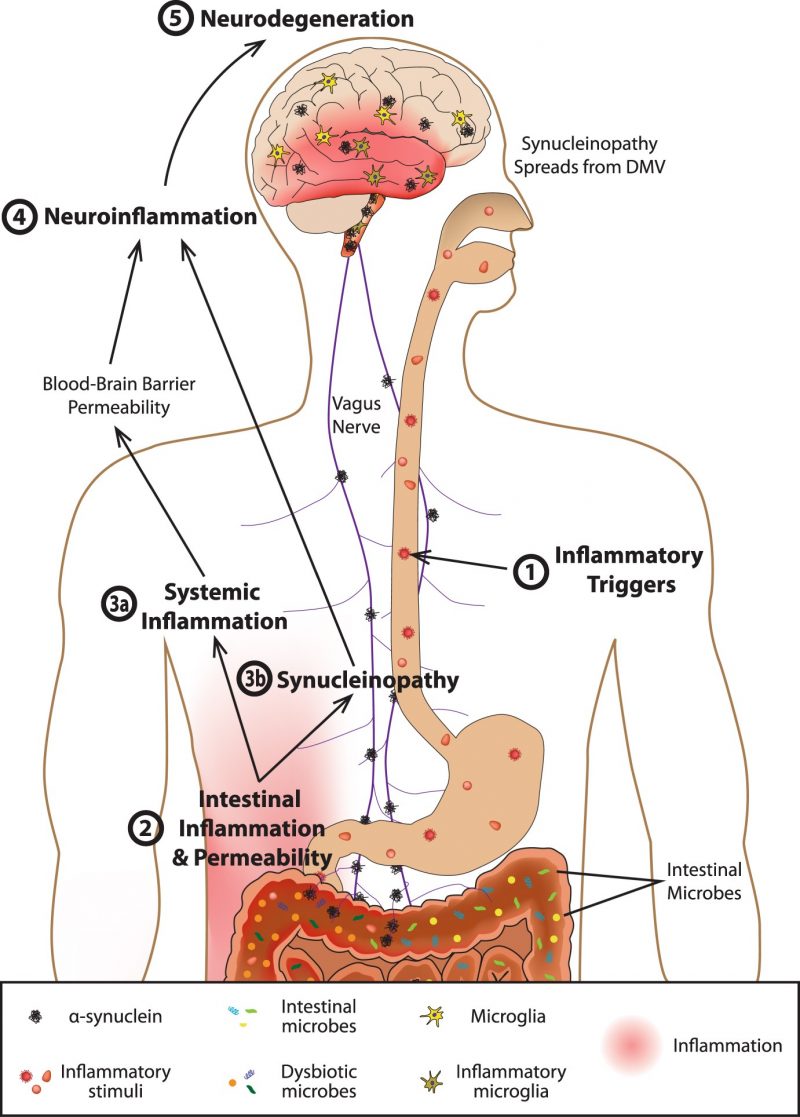
 lead to chronic inflammation and ultimately neuron damage and death. The popular term “leaky gut” may play a role in how inflammation even develops within the brain. The gut-blood barrier is very important inside of the body, which prevents things such as undigested food, toxins, and pathogens from crossing over from the GI tract into blood vessels that can then be carried anywhere within the body via the circulatory system.
lead to chronic inflammation and ultimately neuron damage and death. The popular term “leaky gut” may play a role in how inflammation even develops within the brain. The gut-blood barrier is very important inside of the body, which prevents things such as undigested food, toxins, and pathogens from crossing over from the GI tract into blood vessels that can then be carried anywhere within the body via the circulatory system.