

We learn by watching others. As we grow and develop, we learn how to speak, behave, and even think based on our observations of other humans. Much of this learning is dependent on a part of the brain known as the mirror neuron system. But what happens when the mirror breaks? Read on to find out how this system works and how its dysfunction may contribute to symptoms of ASD.
ASD on the Brain
Autism spectrum disorder (ASD) is diagnosed in roughly 1 in 68 children as of 2017. ASD is characterized by a triad of symptoms: 1. impaired social interaction, 2. language difficulties, and 3. stereotypical (repetitive) behavior.
Many theories have been raised to suggest what causes ASD in the brain. As of yet there is no definitive, accepted, all-encompassing theory. However, most prevalent modern theories boil down to four abnormalities on the neuronal (brain cell) level: synapse construction, impaired protein turnover, impaired regulation of protein expression, and structural modification. Let’s define those terms and take a look at how they’re implicated in ASD.
Synapse Construction
- Synapses are the spaces between neurons. If one neuron sends a signal to another, the chemicals (known as neurotransmitters) that transmit the signal have to cross over the synapse between them.
- In ASD, the brain has many more neurons than expected. Normally, the brain prunes (gets rid of) extra neurons that are not being used. This way the neurons aren’t wasting energy and resources that could instead be used to strengthen connections among neurons that often communicate with one another.
- With the elevated number of neurons in ASD, the connections are not as strong, and there is a lot of extra ‘noise’ from connections that are not necessarily needed.
Impaired Protein Turnover
- Learning occurs due to a process known as long-term potentiation (LTP) in the brain that semi-permanently strengthens connections among neurons. In order for LTP to occur, expression (creation) of certain proteins needs to occur. Creation of these proteins is dependent on a signaling pathway known as the mTOR pathway.
- In ASD, there may be an impairment in the mTOR pathway, resulting in interruptions in LTP and learning.
- mTOR is also important in pruning neurons, so impairment in the pathway could impact synapse construction as well.
Impaired Regulation of Protein Expression
- As explained above, correct levels of protein expression are essential for all of the brain’s functions. Protein expression is dependent on genes; DNA in genes is ‘read’ and transcribed to make proteins.
- Epigenetics is the process of genes being modified by environmental factors. If genes are methylated, methyl molecule groups are added to them, and these block the gene from being read. Methylation is important so that genes coding for development stop being read and transcribed, but too much methylation can silence genes that should be being transcribed into proteins. Epigenetics have been proposed as a factor in causing ASD as environmental factors may impact development.
- Hundreds of gene defects have been found to result in autism, but there is no one ‘autism gene’. Some impacted genes have been found to affect synaptic growth while others impact synaptic transmission (communication among neurons). The problem seems to involve the suppressors of these genes being incorrectly expressed.
Structural Modification
- Altered synaptic activity due to reasons explained above may cause demands that physically change the synapse’s structure such as altered numbers of ion channel receptors (receptors that react to neurotransmitters to let electrically charged ions into and out of the cell).
- Reelin is a gene that plays an important role in organizing the brain and making sure neurons are where they need to be during development. Mutations in the reelin gene have been implicated in ASD.
Phew; that was a (maybe not so) brief overview of neuronal differences that have been found in ASD. Causes of these abnormalities have been theorized, as mentioned in some of the bullet points: genetic and environmental causes have been theorized, as has inflammation. We’re going to look into a recent theory of what might be causing some of those above molecular changes and the symptoms of ASD: the mirror neuron system.
Mirror Neurons
So, what are mirror neurons? First of all, they’re normal neurons with specific functions. Many mirror neurons are located in the motor cortex of the brain, which involves motion, and fire when the body does a specific action. Others are in the somatosensory cortex, which involves pain and sensation, and are activated when touching something or experiencing pain. However, what makes mirror neurons special is that they don’t just activate when you move or feel pain; they also activate the exact same way when you observe another person moving or feeling pain. This ‘mirroring’ activation is important in learning and empathy.
 The mirror neuron system has a wide variety of functions when working normally. It develops in infants before they have reached 12 months of age and begins to let them understand others’ actions. As the famous Hebbian theory of neuroscience states, “cells that fire together, wire together”. This means that cells that are activated simultaneously form connections. This is also known as associative learning as it results in the brain forming an association between the two objects or concepts (for example, a glass of water and the feeling of thirst). Language development, which is in some ways a form of associative learning, also involved this system.
The mirror neuron system has a wide variety of functions when working normally. It develops in infants before they have reached 12 months of age and begins to let them understand others’ actions. As the famous Hebbian theory of neuroscience states, “cells that fire together, wire together”. This means that cells that are activated simultaneously form connections. This is also known as associative learning as it results in the brain forming an association between the two objects or concepts (for example, a glass of water and the feeling of thirst). Language development, which is in some ways a form of associative learning, also involved this system.
Mirror neurons have also been implicated in intention understanding; the deductive understanding not just what a person is doing (drinking a glass of water) but why they are doing it (that person must be thirsty). Mirror neurons are often involved in emotions and empathy as they system allows us to understand and relate to fellow humans. Finally, the mirror neuron system is important in what is known as the theory of mind, being able to imagine what another person is thinking or feeling on a more nuanced level than simple intention understanding.
The ‘Broken Mirror’ in ASD
 With that brief introduction, we can see that the mirror neuron system is quite important in many higher-order brain functions like language, learning, and empathy and that issues with the system could result in significant developmental problems. The “broken mirror” mirror neuron theory suggests that an issue in this system is the cause of ASD. The theory posits that problems with dendritic morphogenesis (the shape of a neuron’s dendritic spines, an area that forms the receiving end of the synapse) resulting from synapse-related causes mentioned above are a large factor contributing to ASD.
With that brief introduction, we can see that the mirror neuron system is quite important in many higher-order brain functions like language, learning, and empathy and that issues with the system could result in significant developmental problems. The “broken mirror” mirror neuron theory suggests that an issue in this system is the cause of ASD. The theory posits that problems with dendritic morphogenesis (the shape of a neuron’s dendritic spines, an area that forms the receiving end of the synapse) resulting from synapse-related causes mentioned above are a large factor contributing to ASD.
Evidence for this theory is found in the fact that the mirror neuron system doesn’t activate the same way in ASD as it does in the non-ASD brain. As mentioned above, the mirror neuron system typically activates in the exact same way when you complete an action and when you observe another person complete that same action. In individuals with ASD, the mirror neurons activate when they complete the action, but not to the same extent when observing another person do so. It’s not all-or-nothing; the system typically still activates, and some studies have found that there isn’t a significant difference since there is so much variability, but on average there is less activation in the ASD brain.
When we consider all the functions that the mirror neuron system is responsible for, it makes sense that abnormalities could be blamed for ASD symptoms including difficulty with language, self-identification, imitating others, and intention understanding. The theory remains far from conclusive and more research needs to be done to find the role that the mirror neuron system plays in ASD, but for now, it presents a compelling theory for what could be causing ASD symptoms: a broken mirror.



 unfortunately still be somewhat difficult to diagnose from a very young age, and so if we as humans have issues diagnosing it within ourselves, it could be even more difficult to actually pin down when observing an animal.
unfortunately still be somewhat difficult to diagnose from a very young age, and so if we as humans have issues diagnosing it within ourselves, it could be even more difficult to actually pin down when observing an animal.  discover similarities in a breed of dog called Bull Terriers, which they found to display some of the (dog equivalent) behaviors that can be diagnosed as autism in humans. I say “dog equivalent” because some of the staple behaviors of ASD are very difficult to distinguish in animals that can’t talk, such as imparied social interaction and not being able to communicate properly, which in humans can manifest as an inability to formulate speech or something similar.
discover similarities in a breed of dog called Bull Terriers, which they found to display some of the (dog equivalent) behaviors that can be diagnosed as autism in humans. I say “dog equivalent” because some of the staple behaviors of ASD are very difficult to distinguish in animals that can’t talk, such as imparied social interaction and not being able to communicate properly, which in humans can manifest as an inability to formulate speech or something similar.  just the behavioral aspect of autism with animals, but also potentially the physiological side of things too.
just the behavioral aspect of autism with animals, but also potentially the physiological side of things too. 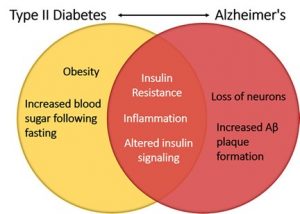






 potential treatment for both diseases, and luckily, scientists are working on this! Inhibiting PTP1B would result in no or less inhibition of insulin signaling, leptin receptors, and calcium channels even under endoplasmic reticulum stress. This would help to decrease the chance of developing type II in AD patients as well as decrease any neurodegenerative symptoms caused by PTP1B caused inhibition. But, it has been deemed an extremely difficult task due to the fact that the active site on PTP1B that an inhibitor would attached to is shared by over 100 other “family members” of this molecule. This makes it difficult for the inhibitor to only effect PTP1B and not any other PTPs present in other parts of the body.
potential treatment for both diseases, and luckily, scientists are working on this! Inhibiting PTP1B would result in no or less inhibition of insulin signaling, leptin receptors, and calcium channels even under endoplasmic reticulum stress. This would help to decrease the chance of developing type II in AD patients as well as decrease any neurodegenerative symptoms caused by PTP1B caused inhibition. But, it has been deemed an extremely difficult task due to the fact that the active site on PTP1B that an inhibitor would attached to is shared by over 100 other “family members” of this molecule. This makes it difficult for the inhibitor to only effect PTP1B and not any other PTPs present in other parts of the body.
 In The Brain
In The Brain However, like stated previously, in AD the insulin signaling is interrupted. This interruption happens because of activated, malfunctioning macrophages. Macrophages play an important role in the immune system and cell death. These macrophages secrete proinflammatory cytokines, which are chemicals that cause inflammation. One important proinflammatory cytokine in AD is called TNF-α. High concentrations of TNF-α cause significant inflammation, which interrupts the insulin signaling pathway, by preventing insulin receptors from activating IRS1 and IRS2 phosphorylation. Therefore, TNF-α causes insulin resistance, ultimately affecting learning and memory.
However, like stated previously, in AD the insulin signaling is interrupted. This interruption happens because of activated, malfunctioning macrophages. Macrophages play an important role in the immune system and cell death. These macrophages secrete proinflammatory cytokines, which are chemicals that cause inflammation. One important proinflammatory cytokine in AD is called TNF-α. High concentrations of TNF-α cause significant inflammation, which interrupts the insulin signaling pathway, by preventing insulin receptors from activating IRS1 and IRS2 phosphorylation. Therefore, TNF-α causes insulin resistance, ultimately affecting learning and memory.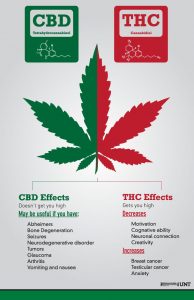 CBD Vs. THC?
CBD Vs. THC?