The Good – A snack
I recently opened the door to my refrigerator and delightfully found a tub of ice cream waiting, practically begging to-be consumed. A smile crept across my face as I pulled the tub out of the freezer for the third time that day when suddenly I remembered an article we had read in my neurochemistry course on Alzheimer’s disease and inflammation. The smile quickly faded, and the ice cream was placed back into the freezer. What does inflammation have to do with Alzheimer’s and how does that have any relevance to my third bowl of ice cream in an afternoon you may ask. I’m here to tell you, more than you think.

The Bad – Alzheimer’s
Alzheimer’s disease is a neurodegenerative condition characterized by loss of memory and other important mental capacities. These malfunctions occur as a result of decreased brain cell connections due to neuronal cell death. Neurons contain a diverse array of cellular machinery and proteins significant to their health and proper functioning. Two of the primary issues in Alzheimer’s are neurofibrillary tangles and beta-amyloid plaques. These result due to issues with the proteins tau and beta-peptide oligomers both of which accumulate and coagulate resulting in neuron and tissue death. The tissues die because coagulation of these proteins blocks the movement of materials inside the cells and the transmission of signals outside and amongst the cells leading to a total loss of function and degeneration of the neurons. But how does that relate to inflammation?

The Ugly – Inflammation
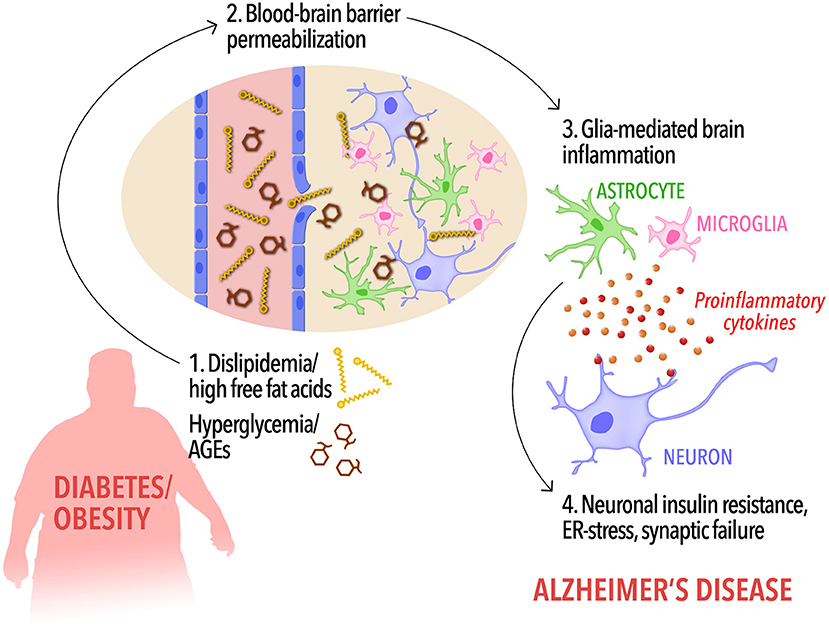
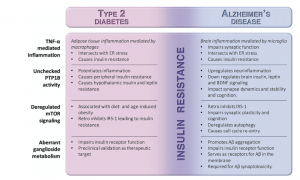
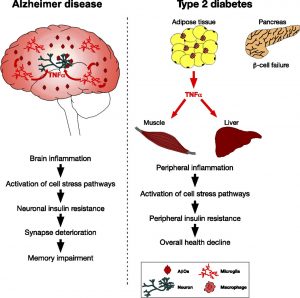
Inflammation specifically chronic low-grade inflammation of tissues recruits cells from the immune system called macrophages (in the body) and microglia (in the brain). This inflammation results in increased activity of a protein abbreviated as PTP1B which has the role of dephosphorylating (deactivating in most cases but not all) other proteins and signaling pathways. This deactivation of important proteins such as IRS1 & IRS2 prevents them from enacting their functions of blocking the over activation of another protein abbreviated as mTOR. When mTOR signaling is improperly regulated then beta-peptide oligomers and tau turn into neurofibrillary tangles and beta-amyloid plaques which develop through a continued long and complex scheme of further improper signaling. MTOR malfunction also leads to insulin resistance which is at the sole of Alzheimer’s disease and its development.
– Insulin Resistance
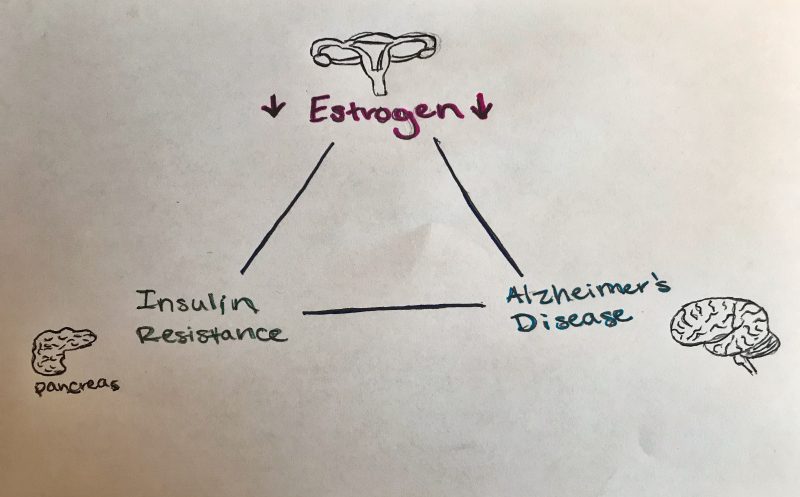
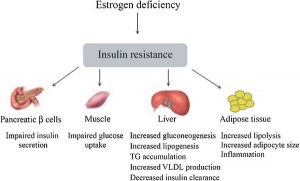
Insulin is a hormone produced in the pancreas (and brain in small quantities) that plays several important roles both within the body and within the brain. Within the body, insulin regulates the metabolism of carbohydrates, fats, and proteins by promoting the absorption of glucose from the blood. Its resistance is the primary cause of type 2 diabetes. Within the brain, insulin plays a neuroprotective role, regulates synaptic plasticity, long-term memory consolidation, and participates in regulating neuron growth and survival. Insulin resistance within the brain leads to neuron vulnerability, degeneration, and Alzheimer’s disease. Because of insulins diverse and significant roles, having type 2 diabetes puts one at risk for developing Alzheimer’s disease and vice versa.

The Ice Cream
Okay that all makes sense (inflammation leads to beta-amyloid plaques, neurofibrillary tangles, and insulin resistance which causes Alzheimer’s disease) but what relevance does ice cream have? A healthy diet is important and can have a positive impact on the prevention of developing multiple conditions including Alzheimer’s disease and type 2 diabetes. A poorly balanced diet, especially one high in fat can stimulate the body to increase its fat stores. It’s this increase in fat storage that recruits immune cells resulting in inflammation and initiating the cascade of events leading to said conditions. Of course, eating ice cream responsibly is of no concern and certainly won’t lead to the development of type 2 diabetes or Alzheimer’s disease in the average individual, but a consistent pattern of poor diet and numerous other factors such as lack of exercise could contribute to an increased risk of development. There remains much to learn about the link between insulin resistance, type 2 diabetes, and Alzheimer’s disease including Alzheimer’s cause and possible treatment strategies. But, with the knowledge we do have, we can be proactive in an effort to best protect ourselves and those we love. Thanks for reading.
Sources


 When functioning normally, insulin in the brain binds to insulin receptors located on the neuron’s cell membrane. These receptors, once activated, phosphorylate proteins called IRS1 and IRS2, which means that phosphate molecules are put on the proteins. This in turn activates IRS1 and IRS2 which go off to cause more activation and signaling cascades resulting in insulin’s aforementioned activities in the brain, like facilitating learning and memory.
When functioning normally, insulin in the brain binds to insulin receptors located on the neuron’s cell membrane. These receptors, once activated, phosphorylate proteins called IRS1 and IRS2, which means that phosphate molecules are put on the proteins. This in turn activates IRS1 and IRS2 which go off to cause more activation and signaling cascades resulting in insulin’s aforementioned activities in the brain, like facilitating learning and memory. Definitely not! First of all, Infliximab is not a preventative drug meant to keep you from developing AD or T2D.
Definitely not! First of all, Infliximab is not a preventative drug meant to keep you from developing AD or T2D. 




 effects of rapamycin that was found was that, when intermittently administered, rapamycin led to stem cell regeneration. Considering some of the applications for stem cells, this is an amazing discovery that could have far reaching implications on the future of medicine. And that’s potentially just the tip of the iceberg. Because of the mTOR1 inhibition through rapamycin, it has been found that there is a decreased risk of cancer, since mTOR1 signaling can lead to cell proliferation. Tumor regression has also been observed to occur. It’s also been found that mTOR1 signalling sometimes leads to misfolded proteins. Using rapamycin, inhibiting mTOR1 led to greater autophagy and suppression of protein synthesis, which is important because this means that rapamycin can have neuroprotective effects in not just Alzheimers, but also Parkinson’s Disease and Huntington’s Disease.
effects of rapamycin that was found was that, when intermittently administered, rapamycin led to stem cell regeneration. Considering some of the applications for stem cells, this is an amazing discovery that could have far reaching implications on the future of medicine. And that’s potentially just the tip of the iceberg. Because of the mTOR1 inhibition through rapamycin, it has been found that there is a decreased risk of cancer, since mTOR1 signaling can lead to cell proliferation. Tumor regression has also been observed to occur. It’s also been found that mTOR1 signalling sometimes leads to misfolded proteins. Using rapamycin, inhibiting mTOR1 led to greater autophagy and suppression of protein synthesis, which is important because this means that rapamycin can have neuroprotective effects in not just Alzheimers, but also Parkinson’s Disease and Huntington’s Disease.  Before we all start taking insulin, it’s important to remember however that one of the most consequential aspects of a drug’s effects and effectiveness is the dosage and how often its administration. With rapamycin, the appropriate ratios of both of these factors are still unknown as of yet, but research is being done to try decipher further how to access the perceived positive effects of the drug. It has been seen though that rapamycin doesn’t fully inhibit mTORC1 processes, and so a combination with another treatment would more effectively implement the positive effects of Rapamycin.
Before we all start taking insulin, it’s important to remember however that one of the most consequential aspects of a drug’s effects and effectiveness is the dosage and how often its administration. With rapamycin, the appropriate ratios of both of these factors are still unknown as of yet, but research is being done to try decipher further how to access the perceived positive effects of the drug. It has been seen though that rapamycin doesn’t fully inhibit mTORC1 processes, and so a combination with another treatment would more effectively implement the positive effects of Rapamycin. increase insulin resistance, but the mechanism for why this occurs is speculated to be known (inhibition of mTOR2). Other negative effects included increased hyperglycemia within type 2 diabetes mouse models, and the ability for tumors to start regrowing after treatment with rapamycin stopped.
increase insulin resistance, but the mechanism for why this occurs is speculated to be known (inhibition of mTOR2). Other negative effects included increased hyperglycemia within type 2 diabetes mouse models, and the ability for tumors to start regrowing after treatment with rapamycin stopped.