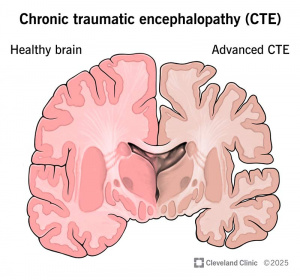
Chronic Traumatic Encephalopathy, commonly known as CTE, is a neurodegenerative disease caused by repeated impacts to the head that lead to devastating mental and physical consequences. People with CTE struggle with emotional problems like aggression, depression and anxiety, cognitive decline and physical decline resembling Parkinson’s (1). But the worst part of CTE is that the victims do not know that they have it, as it can only be diagnosed after death through an autopsy. This leads to misdiagnosis of diseases like Alzheimer’s or Parkinson’s, and a lack of understanding of the behavior of the person with CTE while they are living, often leading to interpersonal troubles. There are currently no treatments for CTE as it is a relatively new concept and there are many questions still unanswered. Therefore, CTE is scary not only because of what it can do to you, but also because there is nothing you can do about it. CTE is devastating disease for patients and their loved ones, that is why you should do everything you can to prevent developing it, and the first step to doing that is to understand how CTE works.
How does CTE work?
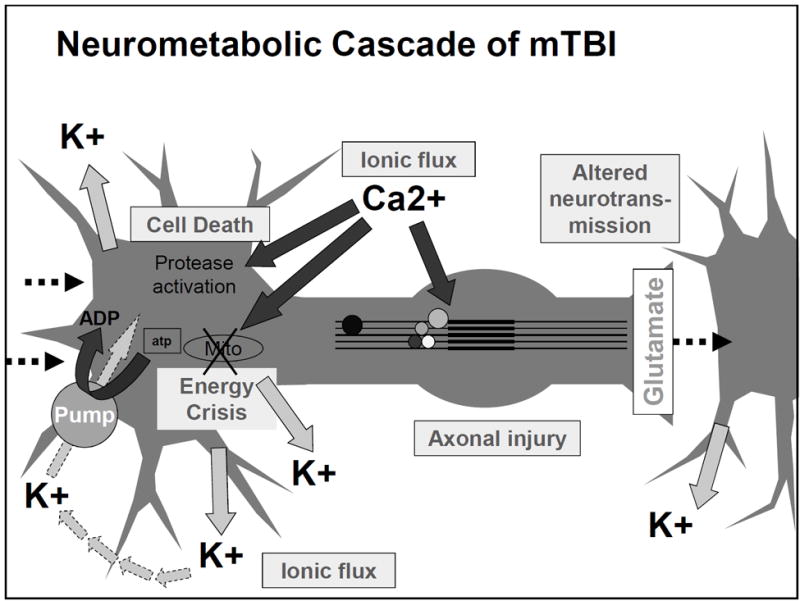
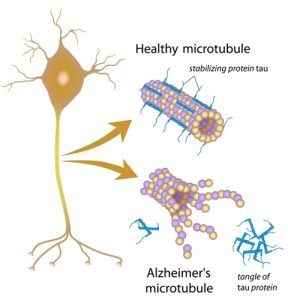
To understand how CTE works we must talk about a protein called tau. This protein is essential to stabilizing the structure of neurons. When someone has repeated head impacts, structures that have tau n them gets stretched out, and our body’s response phosphorylates the tau in the wrong way. When broken down into simpler terms, when you experience a head impact, it causes tau proteins to become loose from the microtubules. Once tau is loose, it is considered pathological, essentially meaning it is not good and can cause disease. Due to the repeated head impacts, this issue with tau phosphorylation never resolves and leads to the spread of disease even between injuries. Eventually, these loose tau proteins start to aggregate together and create something known neurofibrillary tangles, or NFTs for short. These NFTs act as barriers for cellular transport, almost like a spider web that things that are essential for cellular survival get caught in. When this happens, the cell cannot function properly and leads to the starvation of the cell and eventually degeneration and cell death. (2)
What can you do to prevent CTE?
While CTE can develop in anyone, most people who develop it are military personnel who worked with heavy explosives, such as artillerymen, and athletes of contact sports like football, soccer or hockey. Football players are especially at risk, experiencing multiple head impacts every time they play. A study by Boston University examined the brains of football players and found that 99% of former NFL players, 91% of college players and 21% of high school players had CTE. While the study experienced sample bias, with those who donated their brains having shown some signs of CTE rather than a wider population of players, these findings are still extremely alarming.
The only thing you can do to avoid CTE is to avoid head impacts altogether, although this isn’t very realistic for those who play contact sports (3). Finding ways to reduce the frequency of head hits and preventing more impactful hits that result in concussions is essential to avoiding CTE. One study (keep in mind it was not peer-reviewed) conducted by the NFL found that wearing a guardian cap reduced concussions by 50%. Also, making sure your gear is fitted properly is essential to maximizing the force the equipment absorbs. Another way to prevent CTE is to properly recover from concussions. One of the hardest things for an athlete to do it sit out and watch, especially when they feel more or less fine. While you may feel better after a couple days, it takes 2-4 weeks for a concussion to fully recover and returning to action while you are still recovering is not only detrimental for your recovery, but also a risk factor for CTE (4).
Be scared, but not too scared
CTE is a very scary disease for athletes and their parents. While you should definitely do everything you can to avoid repeated head impacts, it is important to remember that everybody experiences a countless number of head impacts throughout their lives. Constantly worrying about every hit your head takes will do you no good. Also, if you are a football player, it can be haunting to hear what CTE is and what it does to you but the majority of people who play football live long and fulfilling lives. It is important to wear protective equipment, wear the equipment properly, and to take the time to recover after getting a concussion. In all, be aware of CTE and its effects, but don’t let it stop you from living your life to the fullest!

- Lakhan, S. E., & Kirchgessner, A. (2012). Chronic traumatic encephalopathy: the dangers of getting “dinged”. SpringerPlus, 1, 2. https://doi.org/10.1186/2193-1801-1-2
- Iqbal, K., Liu, F., Gong, C. X., Alonso, A.delC., & Grundke-Iqbal, I. (2009). Mechanisms of tau-induced neurodegeneration. Acta neuropathologica, 118(1), 53–69. https://doi.org/10.1007/s00401-009-0486-3
- Cleveland Clinic. (2025). Chronic Traumatic Encephalopathy (CTE). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/17686-chronic-traumatic-encephalopathy-cte
- Giza, C. (2021). Recovering from a concussion: 5 tips for your child’s successful healing. UCLA Health. https://www.uclahealth.org/news/article/recovering-from-a-concussion-5-tips-for-your-childs-successful-healing





:max_bytes(150000):strip_icc()/government-job-profile-direct-support-professional-1669627-final-24f90e7cdcb841c3b2954fa4997613dd.png)