
When initially discovered, purified opioids were an exciting and powerful new tool for managing pain. Yet, despite their undeniable effects at alleviating debilitating pain, opioids have progressively fallen out of favor due to their highly addictive properties and lethal side effects. As a result, scientists are beginning the search for opioid-based molecules that retain the analgesic effects of morphine and oxycodone, but abandon the devastating side effects and addictive properties.
According to the CDC, deaths from prescription opioids have quadrupled since 1999 and killed more than 28,000 people in 2014 alone. Additionally, the October issue of Medical Care cited the economic burden of opioid overdose, abuse, and dependence as 78.5 billion dollars per year. Because new drugs would save lives and relieve a major economic burden, research into alternatives for the common opioids are currently being fast-tracked by the FDA.
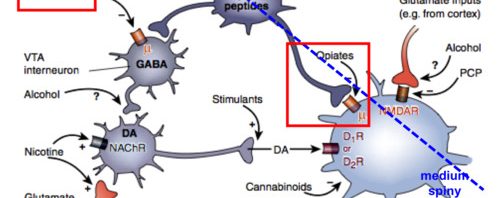
Before the search for these alternatives could begin, more knowledge about the specific receptors for opioids was needed and newfound technologies have made this possible. Three main G-protein coupled receptors exist for opioids, signified as μ, δ, and κ. Research now indicates that the pain relief from opioids results from μ-opioid receptor signaling through the inhibitory G protein, Gi. Interestingly, many of the deadly side effects of opioids, such as respiratory depression, arise from a separate β-arrestin pathway that is downstream from the μ-OR activation.

Efforts are now concentrated on discovering an opioid-like drug that retains the analgesic effects of morphine but lacks the respiratory depression. In essence, the scientific community searches for a μ-OR agonist that elicits a response leading to Gi signaling without a subsequent β-arrestin response.
To find such a molecule, researchers have relied on the crystal structures of the μ-opioid receptor and extensive computer modeling. A research team based at Stanford University computationally docked roughly 3 million known chemical compounds to the μ-opioid receptor. After narrowing the list to around 30 compounds, the team then chemically modified the compound to ensure that it interacted properly with conserved amino acid residues in the receptor’s active site. Finally, they arrived at one molecule in particular which they called PZM21.
From what the researchers have observed thus far, PZM21 could be a life saving drug someday. It has no detectable κ-OR response and 500-fold weaker δ-OR agonist activity. That means PZM21 is a selective μ-OR agonist. Most importantly, however, PZM21 has no measurable recruitment of β-arrestin.
In regard to respiratory depression, morphine heavily depressed respiration frequency compared to PZM21. In fact, the effect of PZM21 was nearly indistinguishable from the negative control. Even a new Gi biased opioid called TRV2130, which is currently in stage 3 drug trials, depressed respiration at 15 minutes. Additionally, PZM21’s length of efficacy is 180 minutes, which is even longer than the maximal dose of morphine.
Another promising finding for PZM21 is its low addictive properties. Along with the lethal side effects of opioids, they are also highly addictive due to increased dopaminergic reward responses in the brain. Research has shown that PZM21 has decreased activation of reward circuits compared to current opioids. Mice taking PZM21 also showed reduced preference to a drug chamber versus vehicle chamber following conditioning.
While PZM21 isn’t ready to be used by humans now, its current successes demonstrate the validity of a structural based approach to G protein coupled receptor ligand discovery. Using the knowledge we have about the biochemistry and structural features of the opioid pathway, we can legitimately search for safer and less addictive, yet still effective analgesics. This in itself is a great scientific accomplishment and one that will hopefully save the lives of many people who would otherwise become addicted to our current opioids.
How Science Can Lead to Safer, Less Addictive Narcotics
















{kind=link}