Marijuana
Marijuana: illegal, euphoria, high, decreased motivation and IQ, munchies, pain and anxiety relief, and potential future medication. These are only some of the many different words and ideas that come to mind when thinking of marijuana. However, as time continues to pass and further scientific research is conducted, we are starting to realize the potential and numerous benefits of marijuana for various illnesses. But how could a recreational drug such as marijuana, still illegal in a majority of states, produce medicinal effects? The answer lies within our own body’s production of endogenous cannabinoids, also known as endocannabinoids, that act upon our body’s cannabinoid system.
The Endocannabinoid System
Endocannabinoids are lipid-based (fatty) molecules made within the body that act upon the cannabinoid system and help maintain homeostasis (stability) throughout the body. These molecules are neurotransmitters (help neurons talk to each other) that are made on demand within the body, and are thus not stored within the body for future use. This allows endocannabinoids to act locally and only for a short time-period for which they are needed to maintain homeostasis within the body.
These molecules act primarily on two known cannabinoid receptors:
CB1 Receptors: the most common receptors; found throughout the central nervous system, peripheral nervous system, and various bodily organs.
CB2 Receptors: less common; found in the immune system and associated tissues (lymph nodes, thymus, spleen, tonsils), as well as the gastrointestinal system.
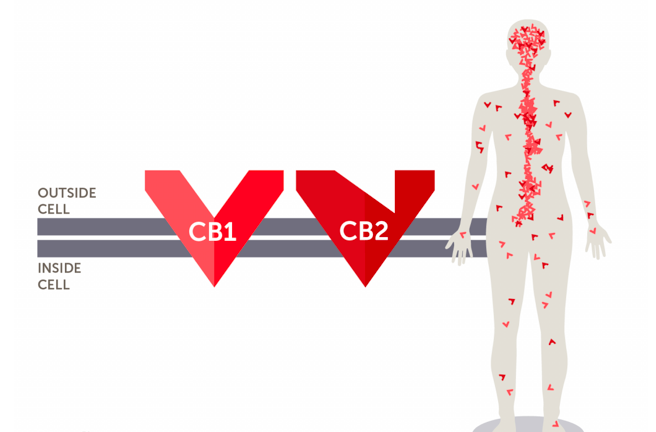
Figure 1. General locations of CB1 and CB2 receptors throughout the body.
The two most highly understood endocannabinoids are anandamide and 2-AG (2-arachidonoylglycerol). Both of these molecules are arachidonic acid derivatives and are formed from lipids in the membrane of cells. These molecules are known as “retrograde neurotransmitters,” meaning that they work backwards. After being created from the cell membrane of a “post-synaptic neuron,” these molecules diffuse backward to a “pre-synaptic neuron,” where they bind to their CB1 and CB2 receptors found within the cell membrane of the “pre-synaptic neuron.”
After binding to their receptors, endocannabinoids lead to a decrease in neurotransmitter release from the “pre-synaptic neuron.” Simply put, endocannabinoids decrease the amount of communication between neurons. In doing so, they often produce inhibitory effects that promote homeostasis, including pain relief, anxiety relief, anti-inflammatory effects, seizure relief, and the death of cancer cells. The endocannabinoids also activate pathways in the post-synaptic neurons from which they were originally made, leading to similar effects as previously mentioned.
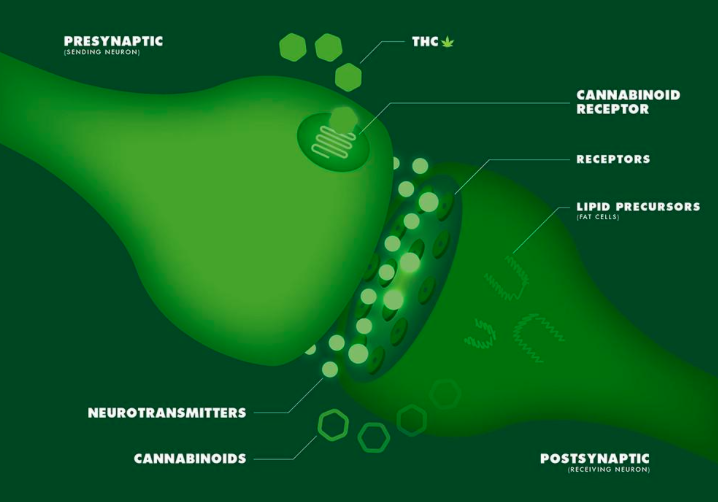
Figure 2. Endocannabinoid synthesis and retrograde action. Actions of THC on cannabinoid receptors.
Marijuana and The Endocannabinoid System
Exogenous cannabinoids, such as those found in marijuana, are known to “supplement” and “enhance” the body’s endocannabinoid system. The commonly known cannabinoid THC has a high binding affinity for CB1 receptors throughout the body. In other words, THC LOVES CB1 receptors and binds to them like a child clings to their mother. When THC binds to CB1 receptors, it has a similar effect to that of natural endocannabinoids binding to CB1 receptors, but the effects are stronger and longer-lasting due to the higher/stronger binding affinity of THC to CB1 receptors. This results in patients experiencing significant relief from pain, nausea, depression, anxiety, and can lead to anti-inflammatory effects.
When THC binds to CB2 receptors, specifically in the gastrointestinal system, it leads to anti-inflammatory responses which offers long-lasting relief to those suffering from Crohn’s Disease and Irritable Bowel Syndrome.
Marijuana: healthy or not?
Marijuana has been proven to have many beneficial and therapeutic effects throughout the body, particularly due to its direct influence on the body’s natural endocannabinoid system that promotes homeostasis.
Therapeutic Effects of Marijuana:
- Pain Relief
- Anxiety Relief
- Seizure Treatment (Epilepsy)
- ADD/ADHD Treatment
- Anti-cancer Treatment (death of cancer cells)
- Stimulates Appetite (for chemotherapy patients)
- Glaucoma Treatment
- Inflammatory Bowel Disease & Crohn’s Disease
- Multiple Sclerosis (severe and persistent muscle spasm treatment)
- the list goes on and on..
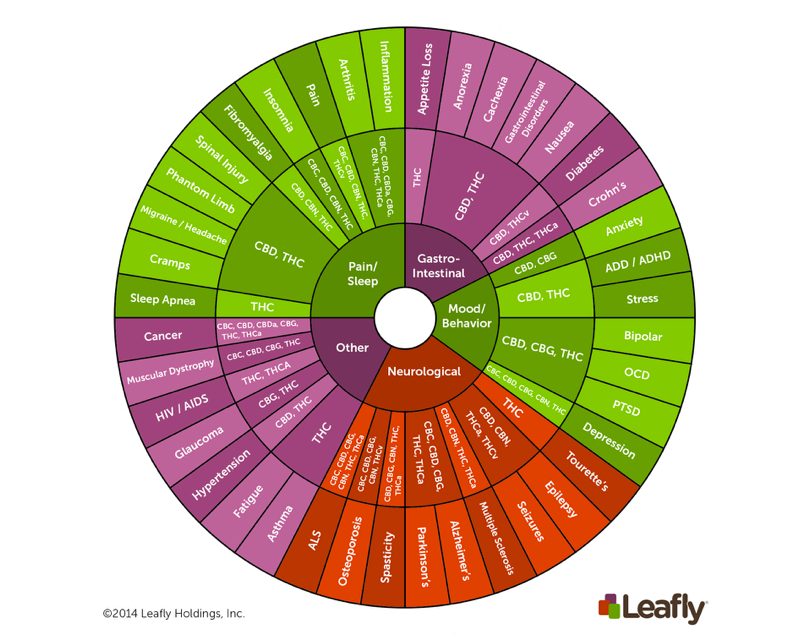
Figure 3. List of various cannabinoids and their corresponding therapeutic effects.
Legalize or Nah?
So, should all 50 states legalize medical marijuana? Should medical marijuana be smoked or orally consumed? Can my current medications be swapped out for medical marijuana instead?
Before confidently answering these questions, much more research needs to be conducted in regard to medical marijuana. Currently, researchers are searching for cannabinoids that offer the same beneficial relief from disease without the psychoactive effects of THC (euphoria, high, mind-altering effects). Wouldn’t it be great to have a new drug that confers the many benefits of marijuana while also allowing you to remain in your own mindset (without the “high”)? This would allow students and those of the workforce to participate in the beneficial effects of the drug while also going about their daily, busy lives.
Unfortunately, due to marijuana’s classification as a Schedule 1 Drug (along with heroine and LSD), it is a very difficult drug to research. There are strict regulations on marijuana that are keeping researchers from accessing the plant, even for scientific use. This is not very convenient being that medical marijuana has shown a lot of promise for therapeutic uses but still needs much more research before being cleared for medicinal use by the FDA.
SO, should we be prescribing medical marijuana? The answer is up to future research and discovery to decide.
For more information regarding the endocannabinoid system’s role in the body and the effects of medical marijuana on the cannabinoid system, please visit:
https://moodle.cord.edu/pluginfile.php/625296/mod_resource/content/0/endocannabinoids.pdf
Figures from:
https://www.leafly.com/news/science-tech/what-is-the-endocannabinoid-system
https://www.vice.com/en_us/article/bnp4bv/how-and-why-your-brian-makes-its-own-cannabinoids
https://www.leafly.com/news/cannabis-101/cannabinoids-101-what-makes-cannabis-medicine